



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























II. Key Components of an In-House NEMT Platform
Building an in-house NEMT platform is not simply about replicating what a vendor offers. It is about creating a system that reflects the unique workflows of your organization, addresses compliance obligations, and ensures seamless integration across the healthcare ecosystem. A well-architected platform should cover every stage of the trip lifecycle, from scheduling and dispatch to billing and reporting. Below are the essential components that every provider should include when designing their own system.
A. Dispatch: Real-Time GPS and Smart Routing
Dispatching is the heartbeat of NEMT operations. Without precision and efficiency, providers face delays, patient dissatisfaction, and higher costs. An in-house dispatch module should include:
- Real-Time GPS Tracking: Live vehicle visibility ensures accurate estimated arrival times and supports compliance with electronic visit verification requirements.
- Automated Routing: Intelligent algorithms should account for traffic conditions, patient mobility needs, and trip urgency to reduce mileage and increase on-time performance.
- Dynamic Adjustments: The system should allow dispatchers to make real-time changes when patients cancel or clinics reschedule.
- Capacity Awareness: For wheelchair or stretcher transports, routing must factor in vehicle capabilities to avoid missed trips or compliance violations.
Providers that own their dispatch logic can continuously refine it, unlike vendors whose updates are delayed by broader customer backlogs.
B. Billing: Medicaid Validation and Automated Claims
Billing is where revenue is either secured or lost. An in-house billing system must be designed with Medicaid-specific requirements in mind, including:
- Eligibility Verification: Automated checks confirm patient coverage before approving trips, thereby reducing the risk of denials.
- Prior Authorization Integration: Built-in workflows capture documentation, track approvals, and flag missing information.
- Automated Claim Submission: Support for formats such as 837P ensures fast, accurate submission to Medicaid and other payers.
- Denial Management: Dashboards should highlight reasons for rejections and allow teams to correct and resubmit quickly.
By owning billing software, providers can align rules to their state’s Medicaid requirements instead of waiting for a vendor patch.
C. Compliance: HIPAA and State-Level Safeguards
Compliance is non-negotiable in healthcare transportation. An in-house NEMT platform must embed compliance by design rather than treating it as an afterthought. Key features include:
- HIPAA Logs and Audit Trails: Every data access or modification should be time-stamped and immutable.
- Protected Health Information Security: Encryption in transit and at rest, along with strict role-based access controls, reduces the risk of breaches.
- State-Specific Requirements: Certain Medicaid contracts require unique trip verification or reporting standards. These should be configurable within the system.
- Incident Response and Monitoring: Built-in workflows for breach notifications and compliance audits strengthen readiness.
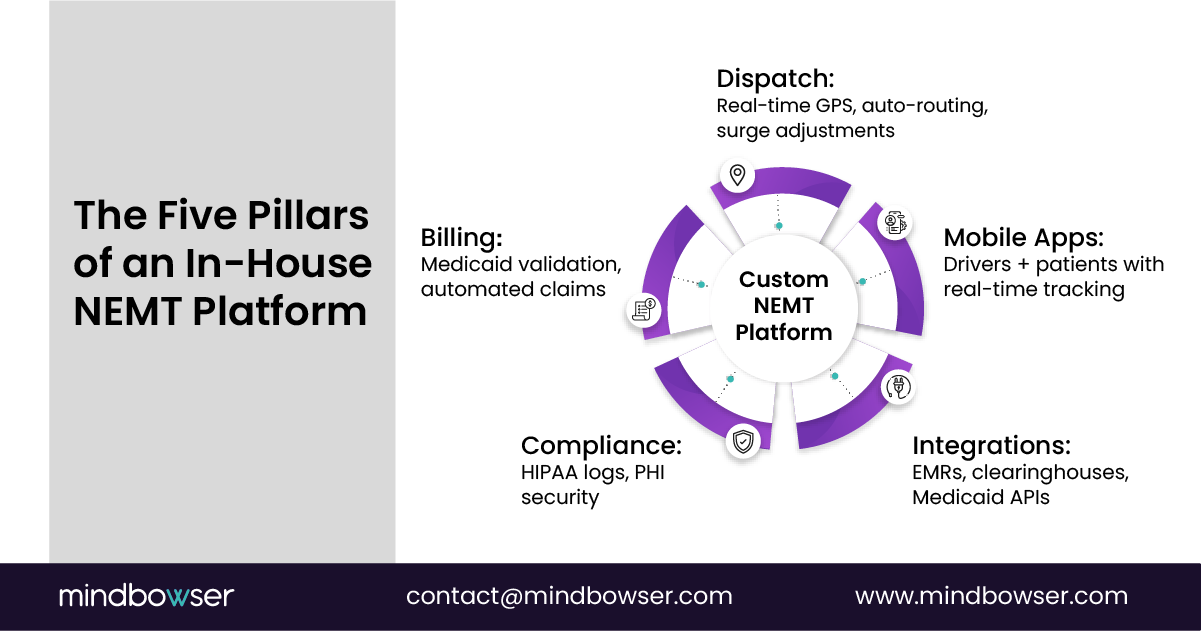
D. Integrations: Connecting the Healthcare Ecosystem
Transportation does not exist in isolation. Hospitals, payers, and brokers all expect integration. An in-house platform should be designed with interoperability at its core:
- Electronic Health Records (EHRs): Integration allows for automated trip scheduling when a provider books an appointment.
- Clearinghouses and Brokers: Direct connectivity simplifies data exchange and ensures faster reimbursements.
- APIs and Webhooks: Open APIs enable future-proof flexibility for new integrations without requiring system rebuilds.
With ownership of the integration layer, providers can respond faster to evolving payer requirements and partnership opportunities.
E. Mobile Applications: For Drivers and Patients
The user experience matters just as much as back-office workflows. A comprehensive platform should include mobile applications tailored for both drivers and patients.
- Driver Apps: Should provide trip acceptance, navigation, proof of delivery through digital signatures or photos, and safety checklists. Offline functionality is important for rural or low-coverage areas.
- Patient Apps: Must include booking, ride reminders, and live trip tracking. Features like feedback surveys improve engagement and satisfaction.
- Caregiver Access: Portals for family members or care coordinators can reduce no-shows and improve communication.
✅ Consultant’s Insight: The most successful in-house NEMT platforms are built around these five pillars. Dispatch and billing protect financial sustainability, compliance ensures long-term security, integrations enable partnerships, and mobile apps elevate patient experience. Together, they form a technology foundation that grows with the provider’s needs, rather than locking them into someone else’s roadmap.
If these costs sound familiar, you’re not alone!
it’s a systemic challenge across NEMT. The good news? Modern technology can stop the leaks before they drain your business. See how Mindbowser helps providers recover revenue and rebuild trust.
III. The Transition Process – Step by Step
Shifting from a third-party NEMT vendor to a fully owned in-house system is a strategic transformation. It requires careful planning, stakeholder buy-in, and phased execution. The good news is that the process can be structured to minimize disruption and deliver measurable results at each stage. Below is a proven roadmap that organizations can follow to replace external platforms with a custom-built NEMT solution.
A. Discovery Phase: Mapping Workflows and Identifying Gaps
The first step is to understand exactly how your organization operates today. Many providers underestimate the hidden inefficiencies in their processes until they are documented.
- Stakeholder Interviews: Engage dispatchers, drivers, billing staff, compliance officers, and even patients to capture pain points.
- Workflow Mapping: Document the process for scheduling, assigning, completing, and billing trips. Identify bottlenecks such as manual entries or duplicate data handling.
- Gap Analysis: Compare current processes with best practices for Medicaid compliance, HIPAA safeguards, and operational efficiency to identify areas for improvement.
Deliverable: A detailed requirements document that highlights what your in-house NEMT dispatch system and billing platform must achieve.
B. Prototype Development: Wireframes and Staff Validation
Once the requirements are clear, the next step is to translate them into early prototypes.
- Wireframes: Design user-friendly layouts for dispatch screens, billing dashboards, and mobile apps.
- Validation Sessions: Share prototypes with frontline staff and gather feedback on usability and user experience.
- Iterative Refinement: Adjust designs based on real-world insights before committing to full development.
This phase ensures that the platform accurately reflects actual workflows rather than assumptions made by leadership or developers.
C. Core Build: Dispatch and Billing Modules First
The foundation of any NEMT system lies in dispatch and billing. These two modules have a direct impact on revenue, compliance, and patient satisfaction.
- Dispatch Core: Build real-time GPS tracking, route optimization, and trip reassignment capabilities.
- Billing Core: Integrate Medicaid validation rules, prior authorization workflows, and automated claim submission.
- Audit Trails: Ensure that both modules generate detailed compliance logs from day one.
Focusing on these areas first delivers quick wins and builds staff confidence.
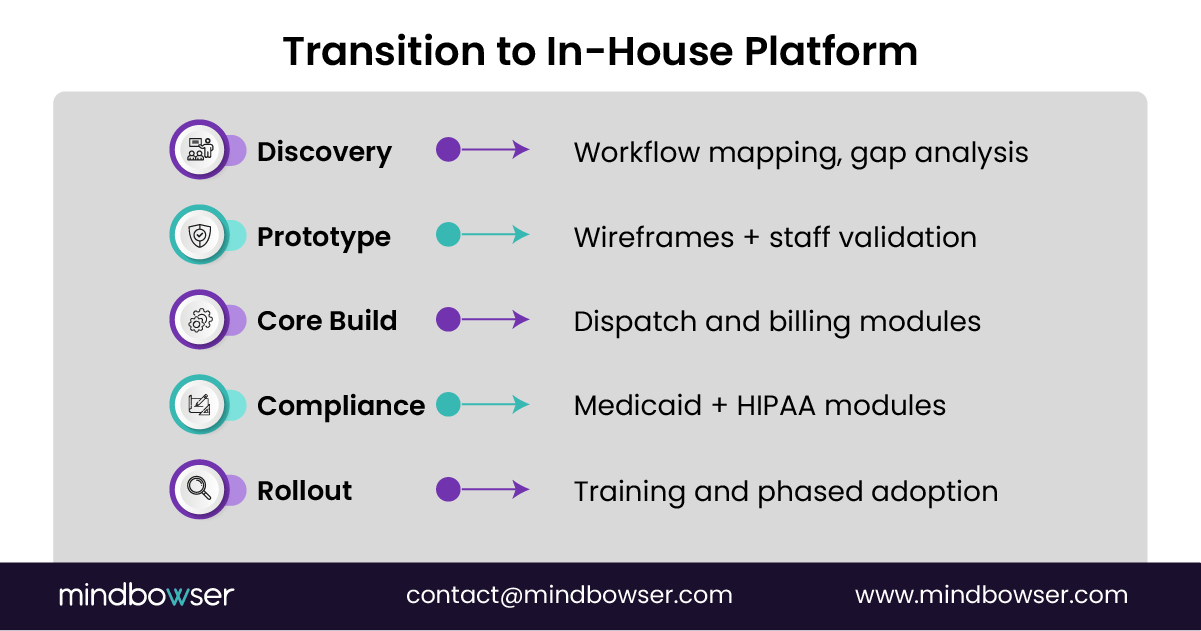
D. Compliance and Medicaid Integrations
With dispatch and billing operational, the next priority is compliance and integration.
- Medicaid APIs: Connect directly with state Medicaid portals for eligibility checks and claim submissions.
- Compliance Safeguards: Embed HIPAA encryption, PHI access logs, and role-based permissions across the system.
- EHR and Clearinghouse Links: Begin integrating with hospital systems and clearinghouses to streamline data exchange.
This phase transforms the system from a scheduling tool into a compliance-ready healthcare platform.
E. Training and Phased Rollout
Technology adoption succeeds only when people are prepared to use it. A phased rollout avoids overwhelming staff and allows for smooth adjustments.
- Training Champions: Identify super users among dispatchers, drivers, and billing staff who can guide their peers.
- Pilot Launch: Start with a subset of vehicles and patient groups, tracking key performance indicators such as on-time performance and denial rates.
- Phased Expansion: Gradually extend the rollout across the fleet, adding patient portals and mobile apps once staff are comfortable.
Deliverable: A fully operational in-house NEMT platform that mirrors your workflows and scales to future needs.
✅ Consultant’s Insight: The transition to an in-house platform is not an overnight project. By breaking it into structured steps, providers minimize risk while building long-term capacity. The focus should always be on aligning technology with workflows, rather than forcing staff to use rigid, vendor-designed systems.
IV. Cost and ROI of Building In-House
Every NEMT provider knows that margins are thin, and financial decisions must be backed by measurable return on investment. The decision to build a custom in-house NEMT platform often raises questions about cost and payback. While there is an upfront investment, the long-term economics and strategic benefits consistently favor ownership. By comparing the total cost of ownership, understanding breakeven timelines, and factoring in the hidden value of intellectual property, providers can make a confident business case.
A. Comparing Three-Year Total Cost of Ownership
Third-party NEMT vendors typically operate on a subscription model with licensing and per-trip fees. At first glance, this seems manageable. However, over the course of three years, these recurring costs far exceed the upfront investment in a custom platform.
- Vendor Model: Licensing fees may range from $1,000 to $5,000 per month, depending on fleet size and trip volume. For a mid-sized provider, this translates to $36,000 to $180,000 over three years. Add per-trip surcharges and integration costs, and the total rises significantly.
- In-House Model: Building a custom NEMT dispatch and billing system may cost $80,000 to $150,000 upfront, plus modest hosting and maintenance fees of $1,000 to $2,500 per month. Over three years, the total investment often equals or undercuts vendor fees, while delivering far greater flexibility and ownership.
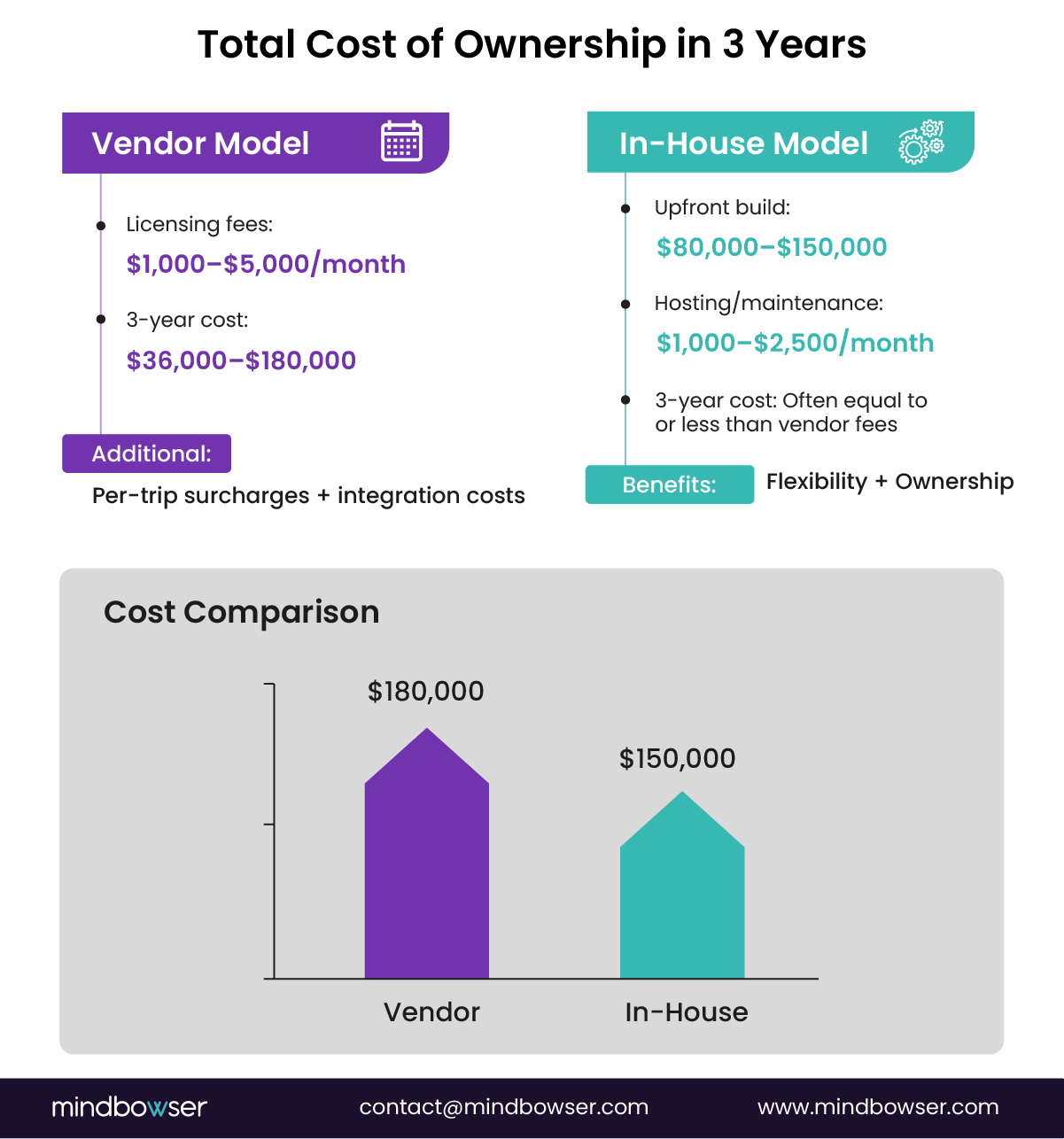
In short, what appears “cheaper” in the beginning becomes more expensive over time when relying on third-party vendors.
B. Breakeven Timelines for Mid-Sized Fleets
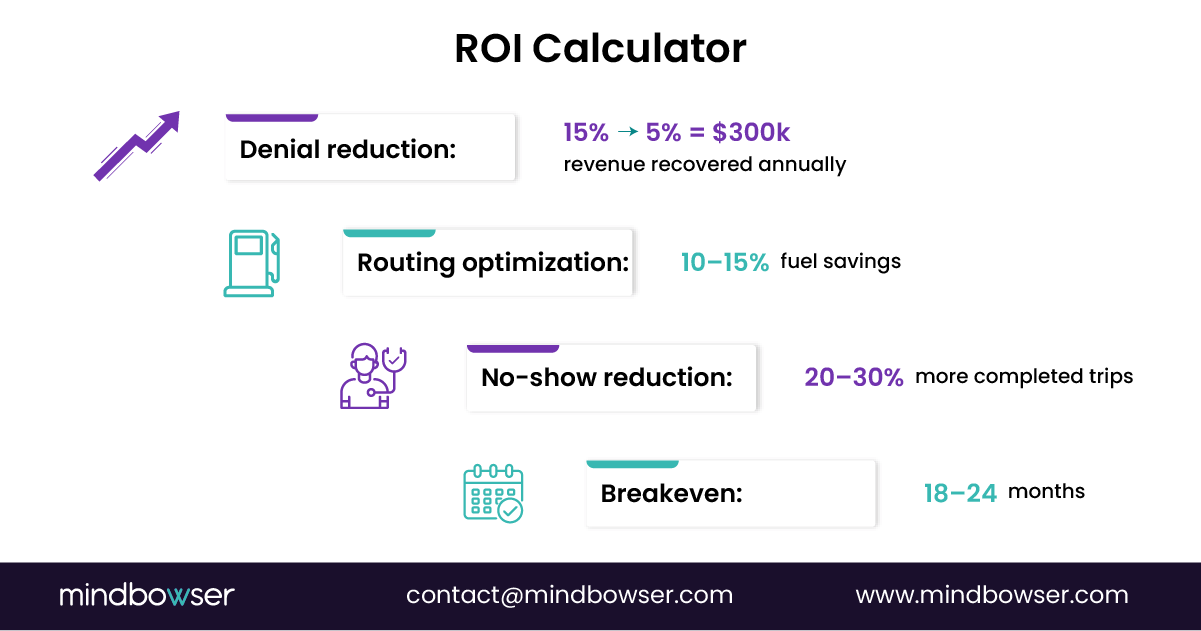
For most providers, the breakeven point for an in-house platform occurs within 18 to 24 months. The reason is that the system not only reduces vendor fees but also recovers revenue that is commonly lost under third-party solutions.
- Claim Denials: With Medicaid-specific validation, denials can drop from 15 percent to below 5 percent. For a provider billing $3 million annually, this can recover $300,000 to $400,000 in lost revenue each year.
- Routing Efficiency: Automated, capacity-aware routing reduces deadhead miles and fuel expenses by 10-15%. For a fleet of 40 vehicles averaging 2,000 miles monthly, that equals more than $40,000 in annual savings.
- No-Show Reduction: Patient portals and reminder systems reduce no-shows by 20-30%, unlocking additional reimbursement without requiring the addition of vehicles or staff.
When these savings are combined, the upfront investment pays for itself quickly and every year thereafter represents pure financial benefit.
C. The Strategic Value of Intellectual Property
Return on investment is not only financial; it also encompasses non-financial benefits. Owning a custom-built NEMT platform also creates strategic value.
- Resale or Licensing Potential: Providers with proprietary technology can license their platform to other operators or even resell it, turning a cost center into a new revenue stream.
- Valuation Growth: Investors view intellectual property ownership as a major differentiator. A provider that owns its dispatch and billing platform commands higher valuations during funding rounds or acquisition negotiations.
- Future-Proofing: Owning the codebase allows providers to adapt continuously. Adding AI-driven scheduling, predictive demand forecasting, or broker integrations can be done on their own timeline, rather than waiting for vendor updates to be implemented.
D. Case for Strategic Control
While the ROI numbers are compelling, the most important benefit of building in-house is strategic control. Providers no longer worry about sudden vendor price increases, delayed compliance updates, or the risk of data lock-in. Instead, they decide the pace of innovation, the scope of compliance, and the roadmap for patient experience improvements.
✅ Consultant’s Insight: The upfront investment in building a custom NEMT platform is best understood as an asset, not an expense. Within two years, most providers achieve breakeven, and within five years, they often enjoy returns exceeding 300%. More importantly, they gain independence, compliance agility, and the ability to grow on their own terms.
V. Common Fears and How to Overcome Them
Even when the advantages of an in-house NEMT platform are clear, many providers hesitate to leap. The hesitation is understandable. Healthcare organizations already operate under tight budgets, heavy compliance requirements, and thin staffing. Building a custom dispatch and billing platform feels like a daunting project. However, most of the fears that surface during the decision process can be anticipated and addressed with a structured approach.
A. Fear: “What if my team cannot handle IT?”
Many NEMT operators lack large technology teams. Dispatchers and billing staff are comfortable with existing tools, and leadership worries that building a custom platform will overwhelm them.
How to Overcome:
- Partner with Healthcare Tech Experts: Instead of trying to do everything in-house, providers can collaborate with technology partners who specialize in NEMT software development. These firms bring healthcare domain knowledge, compliance expertise, and prebuilt frameworks that shorten the learning curve.
- Incremental Rollout: Staff do not need to learn every feature at once. By phasing in modules such as dispatch first and billing later, training becomes manageable.
- Train-the-Trainer Model: Identifying super users among dispatchers and billing staff ensures that internal champions support their peers during the adoption process.
B. Fear: “What if costs spiral out of control?”
Cost overruns are a common concern with custom software projects. Providers fear starting with one budget and ending up with double the expense.
How to Overcome:
- Agile Phases: Instead of building everything at once, projects can be divided into phases with clearly defined budgets and deliverables. Each phase is reviewed before moving to the next, creating financial transparency.
- Minimum Viable Core: Start with the modules that matter most, such as dispatch and Medicaid billing. Enhancements like analytics dashboards or patient portals can be added later.
- Fixed-Cost Contracts: Collaborating with a partner that offers milestone-based pricing helps protect against unexpected overruns.

C. Fear: “Will Medicaid accept my custom system?”
Providers often worry that Medicaid will reject claims submitted through a custom-built platform, leaving them with compliance and reimbursement risks.
How to Overcome:
- Build Compliance from Day One: Custom systems must be designed around Medicaid-specific rules from the start, not added as an afterthought. This includes pre-trip eligibility checks, prior authorization workflows, and support for standard formats like 837P and 835.
- State-Level Certification: Many states require certification or testing before a system can submit claims for reimbursement. Working with a vendor experienced in Medicaid integrations ensures these requirements are met.
- Audit-Ready Logs: Embedding HIPAA audit trails and GPS trip verification ensures that the platform not only meets Medicaid requirements but also positions providers to pass audits with confidence.
D. Fear: “What if my staff resists the change?”
Change management is often overlooked. Even the best technology can fail if staff are reluctant to adopt it.
How to Overcome:
- Involve Staff Early: Bringing dispatchers, drivers, and billing staff into the design and testing process creates ownership and reduces resistance.
- Clear Communication: Leadership should explain how the new system reduces manual work, lowers stress, and helps secure Medicaid reimbursements more reliably.
- Pilot Programs: Running pilots with a small group helps build trust and demonstrates tangible benefits before a full rollout.
VI. Case Study Example
Sometimes the best way to understand the value of moving away from third-party vendors is to see what happens when a provider leaps. The following real-world case illustrates how a mid-sized operator transformed its operations, finances, and compliance posture by building its own NEMT platform.
A. Background
The provider, based in New York, managed a fleet of 60 vehicles and served several counties under Medicaid contracts. For years, they relied on a well-known third-party NEMT vendor to handle dispatch and billing. Initially, the platform appeared sufficient. Over time, however, the cracks began to show:
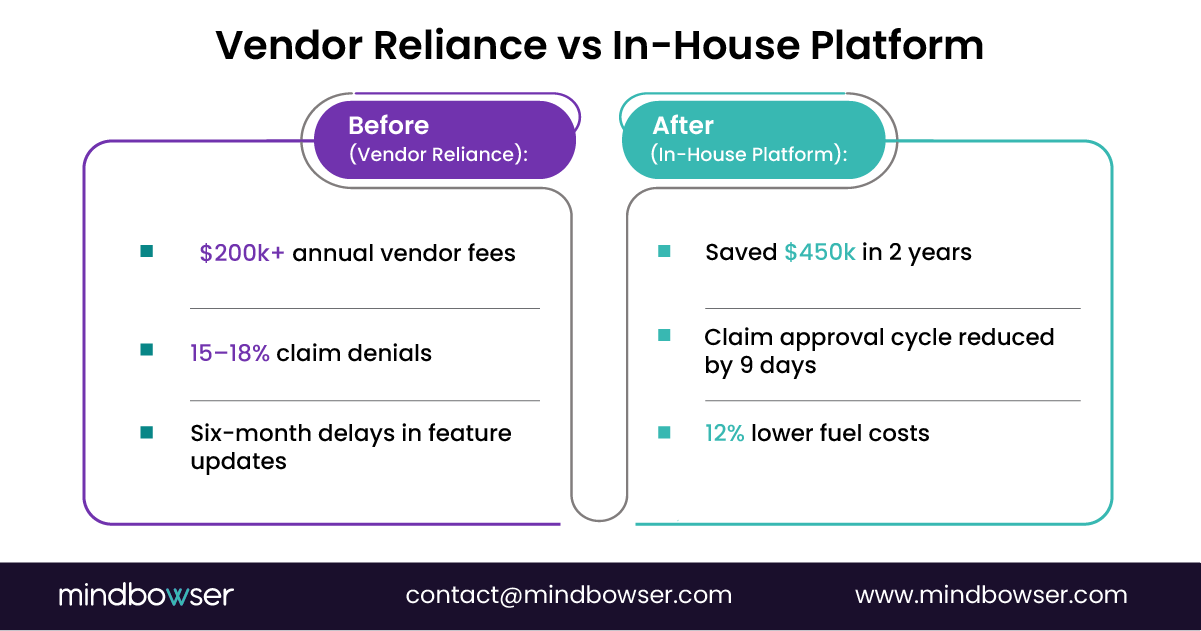
- Licensing and per-trip fees were consuming more than $200,000 annually.
- Medicaid claim rejections averaged between 15% and 18% due to missing state-specific validation rules.
- Updates to the platform were slow, with some integrations taking more than six months to appear.
- Data export was limited, which made it nearly impossible to analyze trends or negotiate with payers from a position of strength.
The leadership team realized that as long as they remained tied to a third-party vendor, they would be reactive rather than proactive in a highly competitive market.
B. Transition to In-House Platform
In 2021, the provider decided to build its own in-house NEMT dispatch and billing system. They partnered with a healthcare-focused technology firm and followed a phased implementation plan:
- Discovery Phase: Mapped workflows, interviewed staff, and documented all state Medicaid billing requirements.
- Prototype Development: Created wireframes for dispatch and billing modules, validated them with dispatchers and billing clerks.
- Core Build: Developed GPS-enabled dispatch with automated routing and built billing modules that incorporated New York Medicaid validation checks.
- Compliance Modules: Added HIPAA audit trails, PHI encryption, and integration with Medicaid APIs.
- Phased Rollout: Started with 15 vehicles as a pilot, trained staff, and gradually expanded fleet-wide within nine months.
C. Outcomes Achieved
The results were significant and measurable within two years:
- Financial Savings: The provider saved approximately $450,000 in vendor fees and recovered revenue lost to billing denials.
- Faster Reimbursements: Medicaid claim approval rates improved, resulting in a 9-day reduction in average payment cycles.
- Operational Efficiency: Optimized routing reduced fuel costs by 12 percent and improved on-time performance scores, thereby strengthening relationships with local hospitals.
- Compliance Readiness: The system generated automated audit logs, which helped the provider pass a Medicaid compliance audit without issue.
- Staff Satisfaction: Dispatchers reported that the new system reduced manual tasks and allowed them to manage more trips per shift without additional stress.
D. Lessons Learned
- Building in-house requires upfront investment but quickly pays off through reduced vendor costs and recovered revenue.
- Staff engagement during design phases ensures smoother adoption.
- Medicaid compliance should be embedded from the beginning, not added later.
- Ownership of data and workflows provides long-term strategic leverage.
See how NEMT Data Dashboards Improve ROI
VII. Why Custom > Off-the-Shelf Forever
For many providers, the choice between off-the-shelf vendor solutions and a custom in-house build feels like a trade-off between convenience and complexity. Off-the-shelf platforms promise quick deployment and lower upfront costs, but they come with long-term limitations. In contrast, custom platforms require a deliberate investment but provide unmatched control, scalability, and ownership. When evaluated over the long horizon, custom platforms consistently prove to be the superior choice.
A. Freedom from Vendor Delays and Roadblocks
Off-the-shelf platforms are designed to cater to the average provider, rather than the unique needs of each organization. As a result, when Medicaid rules change or new features are needed, providers are forced to wait on the vendor’s roadmap. This can result in months of delays while compliance gaps widen and revenue leaks increase.
A custom-built system avoids this trap. Because the provider owns the code, updates can be implemented immediately. Whether it is adding a new Medicaid billing rule, adjusting audit logs, or integrating with a hospital’s electronic health record, changes happen on the provider’s schedule rather than the vendor’s.
B. Elimination of Per-Trip Fees
One of the most overlooked costs in third-party systems is the per-trip fee structure. For providers handling thousands of trips per month, these fees add up quickly and drain margins. Over the course of several years, per-trip fees often exceed the cost of building an in-house dispatch system entirely.
A custom platform eliminates these recurring charges. The more trips a provider delivers, the more cost-efficient the system becomes. This creates scalability that grows with the business, rather than punishing it for success.
C. Scalable Platform That Grows with the Organization
Healthcare transportation is evolving rapidly. What works today may not meet requirements in three years. Off-the-shelf systems are rigid and offer limited flexibility for adding new features, such as artificial intelligence, predictive scheduling, or expanded integrations with payers.
With a custom platform, scalability is unlimited. Providers can begin with core dispatch and billing functions, then gradually add advanced analytics, clearinghouse integrations, or ride-share partnerships. This modular approach ensures that the platform grows in tandem with the organization, making it a long-term asset rather than a temporary solution.
D. Long-Term Financial Advantage
While off-the-shelf systems appear less expensive initially, the cumulative cost of subscriptions, per-trip fees, and missed revenue from claim denials far outweighs the upfront expense of building in-house. By the third or fourth year, most providers realize that their custom platform is not only more cost-effective but also more profitable, as it protects revenue streams that vendors cannot.
E. Strategic Ownership of Data and Intellectual Property
Owning the platform means owning the data and the rules that govern it. With vendor systems, data is often siloed, difficult to export, or tied up in proprietary formats. This creates risk when negotiating with payers, preparing for audits, or considering mergers and acquisitions.
A custom system places full control in the provider’s hands. Intellectual property ownership also opens doors to future revenue opportunities. A provider could license modules to smaller operators, resell the technology, or leverage the platform to negotiate stronger contracts with Medicaid and hospital partners.
Conclusion
The Non-Emergency Medical Transportation sector is at a crossroads. For too long, providers have depended on third-party vendors that offer limited flexibility, recurring costs, and delayed innovation. While these platforms may have provided a stepping stone for digitization, they are no longer sufficient in an environment defined by strict Medicaid compliance, thin margins, and increasing demands for transparency.
Building an in-house NEMT platform changes the equation. Providers that make this move gain complete ownership of their dispatch systems, billing workflows, and compliance safeguards. They no longer wait for vendors to update features or struggle with locked data. Instead, they adapt in real time to state Medicaid rules, integrate directly with hospital systems, and create patient experiences that strengthen trust.
The business case is equally compelling. Within 18 to 24 months, most mid-sized providers achieve a break-even point on their investment. Beyond that point, they enjoy ongoing financial advantages, including elimination of per-trip fees, lower denial rates, and improved cash flow from faster reimbursements. Intellectual property ownership further strengthens valuations, attracts investors, and positions providers as long-term partners in healthcare ecosystems.
Perhaps most importantly, a custom-built NEMT platform empowers providers to control their own future. They decide when to incorporate artificial intelligence for predictive dispatching, when to expand into ride-sharing integrations, or when to enhance patient portals for improved engagement. Instead of being trapped in someone else’s roadmap, they own the path forward.
✅ Consultant’s Insight: In a fragmented market where compliance, efficiency, and patient satisfaction determine survival, technology ownership is no longer optional. Providers that build their own platforms take control of their margins, their contracts, and their destiny.
If your organization is still tied to a third-party vendor, now is the time to evaluate alternatives. Every month of delay means more revenue lost to fees, denials, and inefficiencies.
Thinking of breaking free from third-party vendors? Let us help you build your own dispatch and billing platform.
- Explore how a custom NEMT software development project can align with your workflows.
- Assess whether an in-house NEMT dispatch system would improve on-time performance and compliance.
- Learn how to replace a third-party NEMT vendor without disrupting your operations.
- Discover the financial upside of owning your own NEMT billing software and reclaiming lost revenue.
The future of NEMT belongs to providers who take ownership of their technology. The question is not whether you can afford to build in-house; rather, it is whether you can afford not to. The real question is how much longer you can afford not to.


