



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 



























TL;DR
- Most telemedicine platforms fail due to poor alignment with clinical workflows, not missing features.
- CTOs should focus on integration-first architecture, prioritize core features for MVP, and scale with EHR, RPM, and AI.
- The right feature stack directly impacts provider adoption, patient retention, and long-term ROI.
- Treat telemedicine as a continuous care infrastructure, not just video visits.
Are you building a telemedicine platform or just assembling features that look good in a demo?
Most digital health products struggle not because they lack capabilities, but because those capabilities fail in real clinical workflows.
For CTOs and product leaders, the challenge is not adding more features, but choosing the right ones that drive adoption, efficiency, and outcomes.
This checklist breaks down what actually matters. Not for demos, but for real-world care delivery.
I. What telemedicine software features actually matter for CTOs and product leaders?
A. Why do most telemedicine platforms fail at the feature level?
More features do not mean better outcomes. Yet most telemedicine platforms are built exactly that way.
Here’s the pattern. A product roadmap gets packed with video, chat, AI, dashboards, and alerts. The demo looks impressive. Investors nod. But once deployed, clinicians quietly resist using it.
Why?
Because the platform was built feature-first instead of workflow-first.
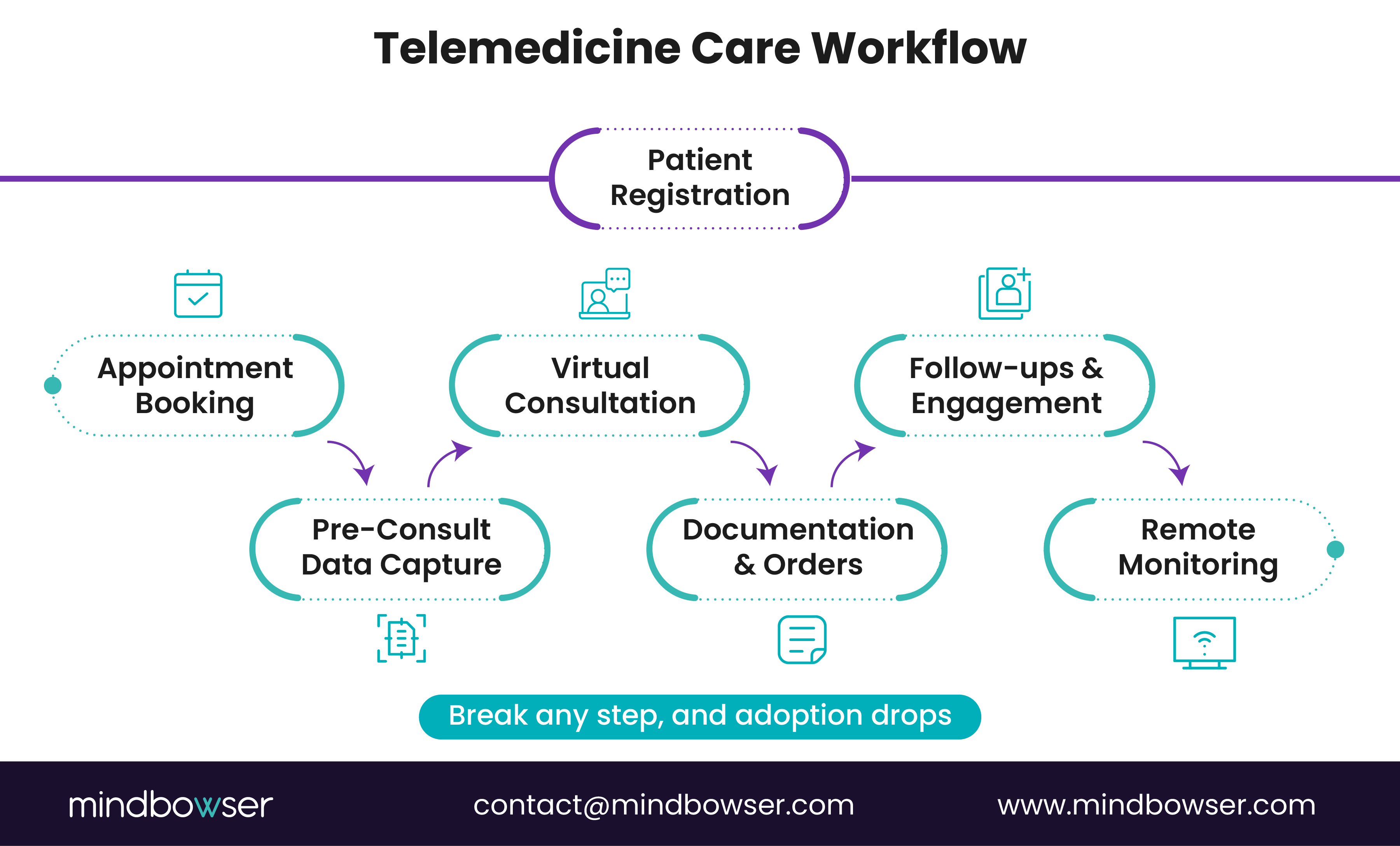
In real care delivery, a provider does not think in “features.” They think in patient flow:
- Intake
- Consultation
- Documentation
- Orders
- Follow-up
If your telemedicine software forces them to jump across disconnected modules, it creates friction. And friction kills adoption. Fast.
Now layer in another issue. Disconnected systems.
Many platforms operate in silos:
- Video lives in one module
- Patient data in another
- EHR somewhere else entirely
The result? Duplicate data entry. Missed context. Frustrated clinicians.
Imagine this scenario:
A physician completes a video consult but must re-enter notes into the EHR manually. Multiply that across 20 patients a day.
That is not inefficiency. That is burnout.
Feature-rich but workflow-poor platforms fail in the real world.
The shift is clear. CTOs must stop asking:
“What features should we build?”
And start asking:
“How does care actually flow, and where does software remove friction?”
That is where successful telemedicine platforms begin.
B. What should CTOs evaluate before defining features?
Before writing a single line of code, CTOs need clarity on care delivery, users, and system dependencies. Skip this step, and even the best feature set will underperform.
Let’s start with the foundation.
1. Care delivery model defines everything
Not all telemedicine platforms are built for the same purpose.
A primary care platform needs:
- High-volume consult handling
- Preventive care workflows
- Simple triage
A specialty care platform needs:
- Multi-party consults
- Imaging and document exchange
- Deeper clinical documentation
Remote Patient Monitoring (RPM) demands:
- Device integrations
- Continuous data ingestion
- Alert-driven workflows
Same “telemedicine.” Completely different feature priorities.
Your feature stack must reflect how care is delivered, not how software is marketed.
2. Who are you really building for?
Telemedicine platforms are multi-user systems:
- Patients
- Providers
- Care coordinators
- Admin teams
Each group has different expectations.
Example:
A patient wants fast access and simplicity.
A provider wants minimal clicks and full context.
A care coordinator wants visibility across journeys.
If one group struggles, the entire system slows down.
This is where many platforms break. They optimize for one persona and ignore the others.
Good products balance all three. Great products connect them.
3. Integration requirements are not optional
This is where most CTOs underestimate complexity.
Telemedicine does not exist in isolation. It must connect with:
- EHR systems
- Billing platforms
- Pharmacy networks
- Device ecosystems
Without integration, teams fall back to manual workarounds.
Ask yourself:
Will providers need to switch systems during a consult?
Will patient data sync automatically across platforms?
If the answer is no, your feature roadmap needs to change.
Define integrations before features, not after.
C. What is the difference between “basic features” and “decision-critical features”?
Not all features carry equal weight.
Some are expected. Others decide whether your platform succeeds or fails.
1. Commodity features vs differentiation layers
Commodity features are table stakes:
- Video consultations
- Appointment scheduling
- Basic chat
Every telemedicine platform has them. They are necessary, but not enough.
Decision-critical features go deeper:
- Integrated clinical workflows
- Real-time EHR sync
- Care coordination tools
These features directly impact how care is delivered, not just how it looks in a demo.
Think of it this way:
Commodity features get you in the game.
Decision-critical features help you win it.
2. Adoption-driving vs demo-friendly features
Some features look impressive but are rarely used.
Dashboards packed with metrics. Complex AI suggestions. Fancy UI layers.
They sell well. They fail quietly.
What actually drives adoption?
- Fewer clicks for documentation
- Seamless data flow
- Context available at the point of care
A CMS-backed insight shows that clinician efficiency improvements of even 10–15% can significantly impact care quality and cost outcomes.
That is where ROI lives.
3. Example: video consult vs integrated care workflow
Almost every platform offers video consults.
But here’s the real question:
What happens before and after the call?
- Is patient history auto-loaded?
- Are notes captured during the consult?
- Can prescriptions be sent instantly?
- Is follow-up care triggered automatically?
If not, the video feature becomes an isolated event rather than a care experience.
And isolated events do not scale into healthcare systems.
Prioritize features that reduce friction across the entire care journey, not just during the consult.
II. What are the must-have core telemedicine software features (MVP checklist)?
A. What features enable seamless virtual consultations?
Virtual care starts with the consult. If this breaks, everything breaks.
At the MVP stage, your goal is not sophistication. It is reliability and clinical continuity.
1. Secure video and audio consultation
This is the backbone. But not just any video.
Healthcare-grade video must deliver:
- Stable connections across low-bandwidth environments
- HIPAA-compliant encryption
- Minimal latency for real-time interaction
A dropped call during a diagnosis is not a minor issue. It is a clinical risk.
According to McKinsey, over 40% of patients cite technical issues as a primary reason for abandoning telehealth platforms.
So yes, video is “basic.” But execution determines adoption.
2. Multi-party conferencing
Care is rarely one-on-one.
You need the ability to bring in:
- Specialists
- Caregivers
- Interpreters
Think of a chronic care patient needing both a physician and a family member present.
Without multi-party support, care becomes fragmented. With it, decisions happen faster and with better context.
This is where simple video evolves into coordinated care.
3. Real-time chat and file sharing
Not everything needs to be said out loud.
Providers often need to:
- Share lab results
- Send instructions
- Drop quick notes
Patients may want:
- Clarifications
- Documents
- Follow-up questions
Real-time chat bridges these gaps.
Consultation features must support conversation, context, and continuity.
B. What features support scheduling and patient flow?
What happens before the consult often determines whether the consult happens at all.
Poor scheduling equals missed appointments. Missed appointments equal lost revenue and care gaps.
1. Appointment booking and calendar sync
Patients expect:
- Self-service booking
- Real-time availability
- Calendar integration
Providers need:
- Clear schedules
- No overlaps
- Easy rescheduling
This is not just convenience. It is operational efficiency.
2. Automated reminders and notifications
No-shows are expensive.
A study using healthcare operations data shows that no-show rates can drop by up to 30% with automated reminders.
Simple interventions like:
- SMS reminders
- Email confirmations
- Push notifications
…drive measurable ROI.
Small feature. Big impact.
3. Queue and triage management
Not all patients need immediate consults.
Some need:
- Triage routing
- Priority handling
- Waitlist management
Without this, providers get overwhelmed, and patients wait longer.
With it, patient flow becomes predictable and manageable.
Scheduling is not a utility layer; it is a revenue and experience driver.
C. What clinical features are required for providers?
If providers struggle, your platform stalls.
Clinical features must reduce effort, not add to it.
1. E-prescriptions and digital orders
Providers need to:
- Prescribe medications instantly
- Send lab orders
- Trigger follow-ups
Anything that requires switching systems slows them down.
Integrated e-prescriptions ensure:
- Faster patient action
- Fewer errors
- Better compliance
2. Clinical documentation and SOAP notes
Documentation is unavoidable.
The goal is to make it:
- Faster
- Structured
- Context-aware
SOAP notes (Subjective, Objective, Assessment, Plan) should be:
- Pre-filled where possible
- Easy to edit
- Linked to patient history
A CDC-backed insight shows that clinicians spend nearly 50% of their time on documentation and administrative tasks.
Reducing this burden directly improves adoption.
3. Patient history and encounter records
During a consult, context is everything.
Providers should instantly access:
- Past visits
- Medications
- Diagnoses
- Lab results
Imagine diagnosing without history. Risky.
This is where telemedicine shifts from transactional to clinical-grade care.
Clinical features must prioritize speed, accuracy, and context.
D. What patient-side features improve onboarding and access?
If patients cannot enter the system easily, nothing else matters.
Adoption starts at onboarding.
1. Easy registration and profile management
Patients expect:
- Quick sign-up
- Minimal data entry
- Secure identity verification
Long forms and friction-heavy onboarding kill conversions.
Would you complete a 10-minute registration for a 5-minute consult?
Most will not.
2. Insurance and payment integration
Healthcare is not just clinical. It is financial.
Patients need:
- Insurance validation
- Transparent pricing
- Smooth payments
Without this, drop-offs increase, and billing becomes chaotic.
Revenue leakage often starts here.
3. Mobile-first experience
Most telemedicine usage happens on mobile devices.
Your platform must:
- Load fast
- Work across devices
- Maintain consistent UX
Mobile is not an add-on. It is the primary channel.
A strong MVP telemedicine platform is not feature-heavy; it is workflow-complete.
III. What advanced telemedicine features differentiate scalable platforms?
A. Why is EHR and interoperability integration critical?
Telemedicine without EHR integration is just a disconnected layer.
At scale, this becomes the single biggest failure point.
Providers already live inside systems like Epic, Cerner, or Athena. If your telemedicine platform sits outside that ecosystem, you force them into duplicate workflows:
- Document in telemedicine
- Re-enter in EHR
- Reconcile data manually
That is not a feature gap. That is a workflow breakdown.
FHIR-based interoperability changes this.
With proper integration:
- Patient data flows in real time
- Notes sync automatically
- Orders and prescriptions align across systems
The real win?
Providers stay in one workflow. Decisions happen faster. Errors drop.
EHR integration is not an enhancement. It is infrastructure.
B. How does remote patient monitoring extend virtual care?
What happens between visits?
That is where most care gaps exist.
Remote Patient Monitoring (RPM) turns episodic care into continuous care.
1. Device integrations (wearables, IoT)
Modern platforms connect with:
- Blood pressure monitors
- Glucose meters
- Wearables
This allows data to flow directly into the system without manual entry.
2. Real-time vitals tracking and alerts
Instead of waiting for the next visit:
- Abnormal readings trigger alerts
- Care teams intervene early
Think post-discharge cardiac patients.
A spike in vitals can trigger intervention before readmission.
3. Chronic care and post-discharge workflows
RPM supports:
- Chronic disease management
- Post-surgical monitoring
- Preventive care
According to the CDC, 6 in 10 adults in the U.S. have at least one chronic condition, making continuous monitoring essential for cost control and outcomes.
This is where telemedicine evolves into population health infrastructure.
RPM shifts care from reactive to proactive.
C. What patient engagement features drive retention and outcomes?
Access gets patients in. Engagement keeps them in.
Most platforms focus on the first. Few solve the second.
1. Messaging, follow-ups, and care reminders
After a consult, patients need:
- Follow-up instructions
- Medication reminders
- Easy communication channels
Without this, adherence drops.
With it, engagement continues beyond the visit.
2. Care plans and education modules
Patients should not leave with just instructions. They need:
- Structured care plans
- Educational content
- Clear next steps
Confusion leads to non-compliance. Clarity drives outcomes.
3. Adherence tracking and nudges
Modern platforms track:
- Medication adherence
- Appointment follow-through
- Behavioral patterns
Then nudge patients with:
- Alerts
- Notifications
- Personalized prompts
That is the scale of opportunity here.
Engagement features directly influence outcomes and retention.
D. How can AI enhance telemedicine platforms?
AI should reduce effort, not add complexity.
When applied correctly, it becomes a force multiplier.
1. AI-powered clinical summaries
During consultations, AI can:
- Capture conversations
- Generate structured notes
- Reduce documentation time
Less typing. More patient focus.
2. Smart triage and symptom checking
Before the consult:
- Patients input symptoms
- AI routes them to the right care level
This reduces unnecessary consults and improves efficiency.
3. Predictive analytics for risk stratification
AI can analyze:
- Patient history
- Vitals
- Behavioral data
To identify:
- High-risk patients
- Potential complications
A McKinsey report estimates that AI could automate up to 30% of healthcare administrative tasks, freeing clinicians to focus on higher-value care.
That is not futuristic. That is operational impact.
AI should remove friction across the care journey.
E. What compliance and security features are non-negotiable?
In healthcare, trust is built on compliance.
There is no shortcut here.
1. HIPAA-compliant data handling
Your platform must ensure:
- Secure storage
- Controlled access
- Data privacy safeguards
Anything less risks legal and reputational damage.
2. End-to-end encryption
All communication must be:
- Encrypted in transit
- Protected at rest
Patients are sharing sensitive data. Security cannot be optional.
3. Audit logs, consent, and access control
You need:
- Full audit trails
- Role-based access
- Patient consent tracking
These are not just compliance requirements. They are operational safeguards.
Security is not a feature. It is a foundation.
Advanced features are not about adding complexity; they are about enabling scale, continuity, and smarter care.
Schedule a Call to Integrate Your Platform With EHRs
IV. How should CTOs prioritize telemedicine features for MVP vs scale?
A. What does a practical MVP feature set look like?
Speed matters early. But direction matters more.
A telemedicine MVP is not about building less. It is about building what proves value fast.
At this stage, your goal is simple:
- Validate adoption
- Enable real consultations
- Capture early feedback
1. Video consult + scheduling + basic documentation
This is your core loop:
- Patient books
- Provider consults
- Notes are captured
If this loop works smoothly, you have a foundation.
If it breaks, adding more features will not fix it.
Think of it as a closed system.
No gaps. No workarounds.
2. Lightweight integrations
Full EHR integration can wait. But some level of connectivity is still required.
Examples:
- Basic patient data sync
- Simple billing hooks
- Exportable records
This ensures your MVP does not become a dead-end system.
3. Fast deployment for market validation
Time-to-market is critical.
A delayed MVP often leads to:
- Missed market windows
- Rising costs
- Stakeholder fatigue
This is where disciplined scope wins.
MVP success = working care loop + early validation.
B. What features should be added for scale and enterprise readiness?
Once adoption starts, the real work begins.
Scaling a telemedicine platform means supporting complexity without slowing down workflows.
1. Deep EHR integration
At scale, Scalable platforms require integration beyond surface-level sync
You need:
- Bi-directional data flow
- Real-time updates
- Embedded workflows within EHR
This reduces duplication and keeps providers inside familiar systems.
2. RPM and care management modules
To move beyond episodic care:
- Add remote monitoring
- Introduce care coordination workflows
- Enable longitudinal patient tracking
This is where revenue models expand into:
- Chronic care management
- Value-based care programs
3. Analytics and reporting dashboards
Leadership needs visibility.
Platforms should provide:
- Utilization metrics
- Clinical outcomes
- Financial performance
What is working? What is not?
Without analytics, scaling becomes guesswork.
Insight drives optimization.
scale requires depth, not just breadth.
C. Feature prioritization framework (decision table)
Not every feature deserves equal investment.
CTOs need a structured way to decide:
- What to build now
- What to delay
- What to avoid entirely
Here is a practical framework.
1. Must-have vs nice-to-have vs differentiators
- Must-have: Enables core care delivery
- Nice-to-have: Improves experience but not critical
- Differentiators: Drives competitive advantage
Misclassify these, and your roadmap drifts.
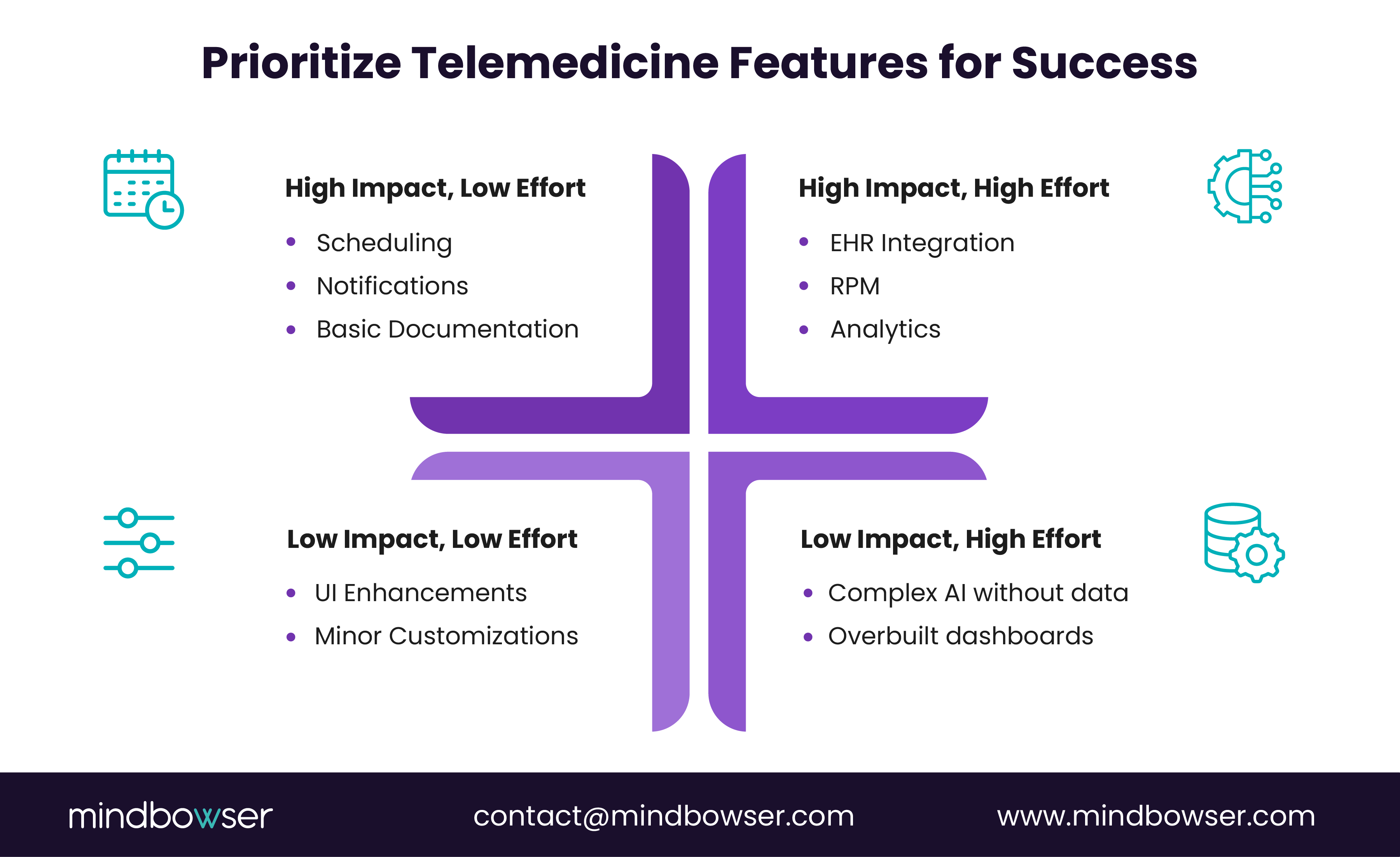
2. Impact vs effort matrix
Evaluate each feature based on:
- Clinical impact
- User adoption impact
- Development effort
High-impact, low-effort features should always come first.
3. Time-to-market vs long-term ROI
Some features:
- Help you launch faster
Others:
- Drive long-term revenue and retention
Balancing both is the CTO’s real job.
Simple decision logic:
- Does it improve care flow? → Build now
- Does it improve the experience only? → Evaluate
- Does it add complexity without a clear ROI? → Delay
Feature prioritization is less about technology and more about disciplined decision-making.
V. Telemedicine software features checklist (CTO-ready table)
A. Core features checklist
This is your non-negotiable baseline. If any of these are weak, adoption will suffer regardless of what you add later.
1. Core consultation and access layer
- Video consultation
- Scheduling and calendar management
- E-prescription capability
- Patient management system
These features form the minimum viable care loop.
If a provider cannot complete a full consult without switching systems, your core is incomplete.
Execution matters more than presence. A stable video experience and fast documentation flow will outperform a feature-heavy but clunky system every time.
B. Advanced features checklist
This is where platforms start becoming scalable systems, not just tools.
1. Integration and continuous care layer
- EHR integration (Epic, Cerner, Athena)
- Remote patient monitoring (RPM)
- Patient engagement tools (messaging, reminders, care plans)
These features enable:
- Longitudinal care
- Reduced clinician workload
- Better patient outcomes
This is where telemedicine transitions into care infrastructure.
C. Differentiation features checklist
This is where competitive advantage is built.
1. Intelligence and workflow acceleration layer
- AI capabilities (clinical summaries, triage)
- Workflow automation (alerts, routing, documentation assist)
- Multi-specialty scalability
These features:
- Reduce operational friction
- Improve decision-making speed
- Support expansion across specialties
A McKinsey estimate suggests AI-enabled workflows can significantly reduce administrative burden, improving both cost efficiency and clinician productivity.
But caution.
Do not add these before your core and advanced layers are stable.
Otherwise, you are layering intelligence on top of broken workflows.
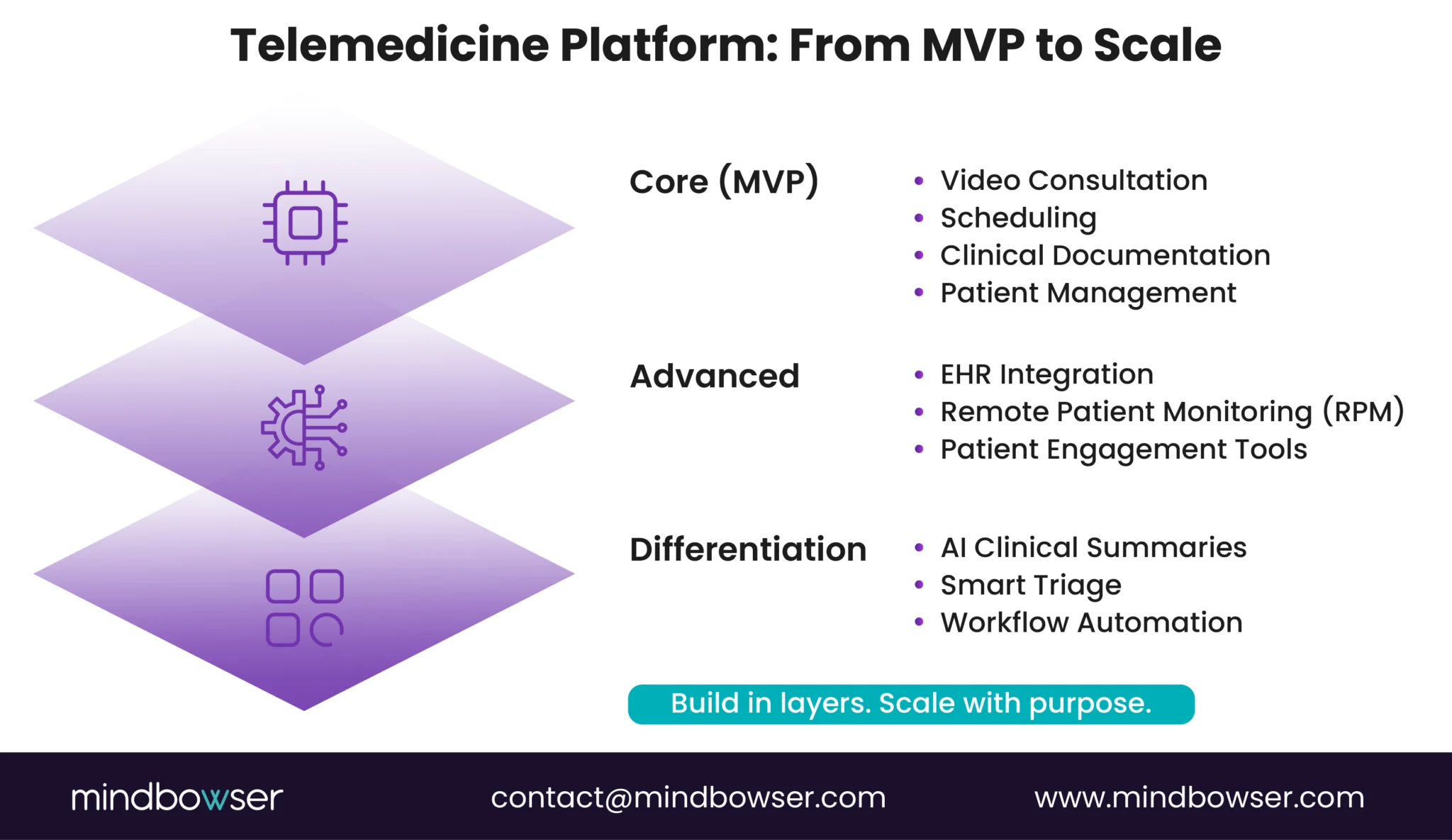
Quick decision snapshot:
- Core = Enables care
- Advanced = Extends care
- Differentiation = Accelerates and scales care
A strong telemedicine platform is built in layers, not all at once.
VI. How Mindbowser helps build telemedicine platforms that scale
A. Why custom telemedicine development matters for CTOs
Off-the-shelf platforms look fast. They rarely stay flexible.
At first, they help you launch. Then reality sets in:
- Limited integrations
- Rigid workflows
- Feature constraints you cannot control
And suddenly, your roadmap depends on someone else’s product decisions.
This is where custom development changes the equation.
1. Avoiding rigid, off-the-shelf limitations
Pre-built platforms force you to adapt your workflows to their structure.
But healthcare workflows are not generic. They vary by:
- Specialty
- Care model
- Patient population
Custom-built platforms adapt to your workflows, not the other way around.
2. Building around workflows, not features
Instead of stitching together disconnected modules, custom builds allow:
- Unified care journeys
- Context-aware interfaces
- Reduced clinician effort
Less switching. Less duplication. More focus on care.
This is where adoption improves. Quietly, but consistently.
3. Faster integration with existing systems
Integration is often the biggest bottleneck.
Custom architectures enable:
- Direct EHR connectivity
- Flexible API layers
- Faster onboarding of new systems
What usually takes months can be reduced significantly with the right approach.
Custom development gives CTOs control over both speed and direction.
B. Mindbowser accelerators and capabilities
Speed does not have to come at the cost of flexibility.
Mindbowser approaches telemedicine with a hybrid model:
- Pre-built accelerators for faster launch
- Custom architecture for long-term scale
1. HealthConnect CoPilot for workflow orchestration
Designed to align with real care delivery:
- Orchestrates patient journeys
- Connects multiple systems
- Reduces manual coordination
This is where workflows become visible and manageable.
2. AI Medical Summary for clinician efficiency
Documentation is a major burden.
This accelerator helps:
- Auto-generate clinical summaries
- Reduce typing effort
- Improve documentation consistency
Less admin work. More patient interaction.
3. RPM integrations for continuous care
Supports:
- Device connectivity
- Real-time monitoring
- Alert-driven interventions
This extends telemedicine beyond visits into ongoing care management.
C. Example outcomes
What does this look like in practice?
1. Improved provider adoption
When workflows align:
- Fewer clicks
- Less duplication
- Faster consult cycles
Providers use the system because it helps them, not because they have to.
2. Faster go-to-market for digital health startups
With accelerators and focused builds:
- MVP timelines shrink
- Validation happens earlier
- Iteration becomes easier
Speed with direction. Not speed alone.
3. Better patient engagement and retention
With integrated care journeys:
- Patients stay connected
- Follow-ups improve
- Outcomes improve
A Deloitte-aligned insight shows that connected patient experiences significantly improve retention and satisfaction.
The right architecture lets you move fast today without slowing down tomorrow.
Why a feature checklist is not enough
A checklist gives coverage, not success. Telemedicine platforms fail when features are disconnected from care delivery, poorly integrated, or add friction instead of removing it. What matters is alignment with real workflows, tight integration with existing systems, and the ability to support continuous care beyond the consult. Build for that, and adoption, outcomes, and ROI follow.
The most important features are secure video, scheduling, clinical documentation, and EHR integration. These ensure smooth care delivery and drive provider adoption.
An MVP should focus on video consultations, appointment scheduling, and basic documentation. This creates a complete care loop for early validation.
Integration happens through APIs and FHIR standards, enabling real-time data exchange and reducing duplicate work for clinicians.
Essential compliance features include HIPAA-ready data handling, encryption, audit logs, and role-based access control to protect patient data.
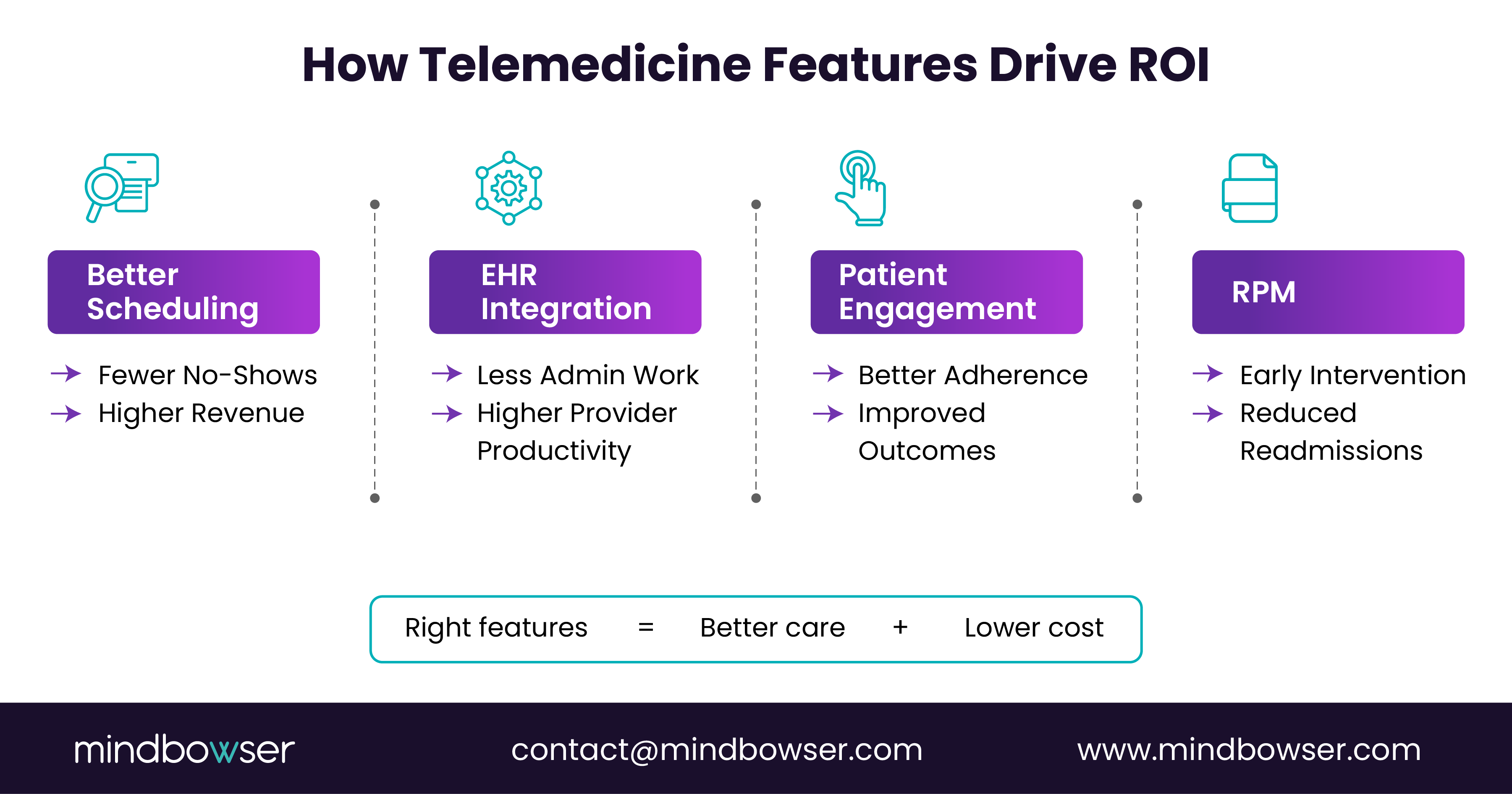
AI and RPM improve ROI by reducing administrative workload, enabling early intervention, and improving patient engagement, thereby lowering long-term costs.


