BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























Can AI agents for nurses really give two hours back per shift without creating compliance risk?
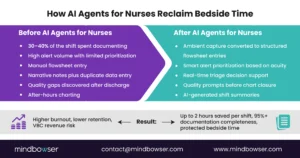
Picture a 7 p.m. shift change. A nurse wraps up bedside care but still has an hour of charting left. Alerts keep firing. Quality fields are buried in the EHR. She stays late. Again.
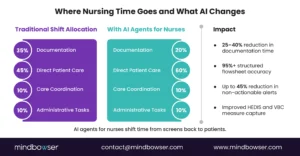
This is the pressure many CNOs face: 30–40% of nursing time lost to admin work, retention under strain, and value-based contracts tied to documentation accuracy.
AI agents for nurses offer a different path. When built into real nurse workflows and integrated directly with structured EHR fields, they can capture ambient conversations, prioritize alerts, support triage, and reduce documentation burden without compromising governance.
The question is not whether to explore AI. It is the AI agents that nurses can safely deliver measurable results fast.
I. Why “AI Agents for Nurses” Is Suddenly an Operations Priority
Ask any CNO: Can AI agents for nurses finally reclaim two hours of documentation time per shift without creating compliance nightmares?
That question is no longer theoretical. It is a budget line item, board discussion, and retention strategy rolled into one.
Nursing leaders face a perfect storm. Between 30 and 40% of a nurse’s shift now goes to administrative tasks, much of it tied to AI nursing documentation inside the EHR [Healthcare IT News]. Retention rates in many systems hover below 80% [Industry reports]. At the same time, quality metrics are wired directly to value-based care contracts. Miss your HEDIS targets. Miss your margin.
AI agents for nurses are moving from pilot curiosity to operational mandate because they promise something rare: time back at the bedside without risking compliance or data integrity. But only when built for nursing realities, not retrofitted from physician workflows.
Let’s unpack why this shift is happening now.
A. The Documentation Tax Is Breaking Throughput
Nurses are charting more than caring. That is the hard truth many CNOs now admit behind closed doors.
Ambient AI pilots reported saving up to 2 hours per shift when documentation is captured and automatically structured into flowsheets. That is not a marginal gain. That is a staffing lever.
Consider the math:
- 2 hours saved per nurse per shift
- 200 bedside nurses
- 365 days
You are looking at the equivalent of dozens of FTEs redirected to direct patient care. No new hires. No overtime spikes. Just better workflow design.
Yet here is the tension. Traditional AI nursing documentation tools often stop at transcription. They generate narrative notes, not structured data. Nurses still click, validate, and reconcile. The “time savings” melt away.
AI agents for nurses change that equation. Instead of chat-based outputs, they deliver:
- Structured flowsheet entries
- Auto-mapped quality measures
- Real-time prompts inside nurse workflows
Short sentence. Big impact.
A Midwest health system piloting nursing AI agents saw documentation time drop while handoff accuracy improved, reducing rework and near-miss anxiety. The emotional lift matters. Burnout is not abstract. It is felt at 6:45 p.m. when charting spills into personal time. Exhaustion. Frustration. Doubt.
Reclaiming documentation time is not about efficiency alone. It is about protecting throughput, morale, and margin in one move.
B. Retention, Quality Scores, and VBC Are Now Linked
Retention is a financial metric. Turnover costs per bedside nurse can exceed $40,000 when you factor in recruitment, onboarding, and temporary staffing. And when retention dips below 80%, quality performance often follows.
Why? Because continuity drives outcomes.
Value-based care contracts tie reimbursement to readmissions, care coordination, HEDIS measures, and patient experience. Many of those metrics depend on nursing documentation accuracy and timeliness. Miss a flowsheet entry. Miss a quality credit.
Here is the conflict.
Nurses are asked to document more for VBC reporting while being told to “spend more time with patients.” The system demands both speed and depth. Humanly, that tension cracks.
AI agents for nurses align retention with revenue. When nursing AI agents:
- Auto-suggest evidence-based interventions
- Flag missing quality data in real time
- Generate concise shift summaries for clean handoffs
They reduce cognitive load while strengthening documentation integrity.
One CNO described it this way: “If I can give my nurses 90 minutes back and improve my quality scores, that is not tech spend. That is workforce strategy.” Relief. Finally.
The triad is clear: documentation burden, burnout, value-based performance. Fix one well, and you influence all three.
C. Chatbots Failed Nurses. Workflow-Native AI Agents Will Not.
Let’s be candid. Early AI tools for clinicians often felt like physician hand-me-downs. Built for dictation. Designed around provider notes and poorly mapped to nursing flowsheets.
Nurses noticed.
Typing into a chatbot that spits out a paragraph is not helpful when the EHR demands discrete data fields, structured assessments, and compliance-ready entries. It creates duplication, not relief.
AI agents for nurses are different. They operate inside nurse triage AI pathways, medication administration workflows, and bedside assessment templates. They:
- Capture ambient conversation
- Convert it into structured AI nursing documentation
- Validate against care protocols
- Log activity for audit readiness
This is ga overnance-first design. And it matters. Regulatory scrutiny around AI in healthcare is rising, especially when outputs influence clinical decisions. CIOs and CMIOs need traceability. CNOs need safety. Everyone needs uptime.
Contrast chatbot novelty with workflow-native reliability. One is interesting. The other is operational.
So the real question is not “Should we explore AI agents for nurses?”
It is “How fast can we deploy nursing AI agents that respect nursing reality, protect compliance, and deliver measurable ROI?”
Because bedside time is finite, and it is sacred.
AI agents for nurses have shifted from experiment to operations priority because they sit at the intersection of staffing, quality, and revenue. Ignore them, and the documentation tax keeps compounding.
II. Practical Use Cases: Where AI Agents for Nurses Deliver Measurable ROI
CNOs do not fund technology. They fund outcomes.
So let’s move past theory. Where do AI agents for nurses actually cut documentation burden, improve throughput, and protect bedside time? Not in generic note generation. Not in dashboards that no one opens. In workflow-native interventions that map directly to nurse tasks.
Below are the six use cases we see driving measurable ROI across mid-market health systems and growth-stage care platforms.
A. Ambient Documentation That Writes to Structured Flowsheets
This is the headline win.
Ambient AI nurses capture bedside conversations and assessments in real time. But unlike first-generation tools, advanced AI agents for nurses convert that audio into:
- Structured flowsheet entries
- Discrete vitals and assessment data
- Quality-tagged documentation for HEDIS and VBC reporting
Healthcare IT pilots report up to two hours saved per nurse per shift when ambient AI nursing documentation is implemented correctly. That time is not just reclaimed. It is redirected to patient interaction, discharge planning, and education.
Short sentence. Massive lift.
The difference is in structure. If your ambient AI stops at narrative text, nurses still reconcile fields manually. Workflow-native nursing AI agents eliminate duplicate entry by mapping outputs directly to EHR schemas.
When AI agents for nurses write directly into structured documentation fields, time savings compound shift after shift.
B. Nurse Triage AI That Reduces Escalations and ED Leakage
Triage is pressure.
Nurses balance symptom assessment, protocol adherence, patient anxiety, and throughput targets. One missed cue can trigger unnecessary escalation. Or worse, a delayed intervention.
Nurse triage AI embedded within AI nurse workflows can:
- Surface evidence-based decision trees in real time
- Flag high-risk symptom clusters
- Suggest next-best actions aligned to protocols
In pilots, triage decision support reduced handling time by approximately 30 minutes per complex case while lowering avoidable ED transfers tied to uncertain escalation.
Here is the contrast. Without AI agents for nurses, triage relies on memory and manual protocol lookup. With workflow-native support, guidance appears in context. Not in another tab. Not in a binder.
One CMIO shared that triage standardization reduced variation across units, improving both safety and confidence. Relief. Consistency. Fewer second guesses.
From a VBC lens, reducing avoidable ED visits and unnecessary escalations directly supports cost-of-care targets. Triage is not just clinical. It is financial.
C. Alert Prioritization to Combat Alarm Fatigue
Alarm fatigue is real.
Nurses can receive hundreds of alerts per shift, many of which are low-value or redundant. Cognitive overload increases error risk and slows response time.
AI agents for nurses can triage the alerts themselves. By analyzing patient acuity, recent interventions, and historical trends, nursing AI agents can:
- Suppress low-priority alerts
- Elevate clinically meaningful changes
- Cluster related notifications into single action prompts
Early results show up to a 45% reduction in non-actionable alarms, with improved response times for true clinical deterioration.
This is not about silencing alarms blindly. Governance matters. AI nurse workflows must log suppression logic, maintain audit trails, and align with compliance frameworks to ensure transparency.
The benefit chain is clear:
Fewer unnecessary alerts → Lower cognitive load → Faster response to real events → Fewer adverse outcomes.
This works. Period.
D. Clinical Summarization for Safer Handoffs
Shift change is a vulnerability point.
Incomplete handoffs contribute to medication errors, missed follow-ups, and delayed interventions. Yet nurses often summarize complex patient states under time pressure.
AI agents for nurses can generate concise, structured shift summaries that include:
- Active problems and risk flags
- Recent interventions and response
- Pending labs, consults, and discharge barriers
When embedded in AI nurse workflows, these summaries pull directly from flowsheets and care plans, reducing reliance on memory.
Pilots report up to 45 minutes saved per shift in documentation and prep time, along with measurable improvements in handoff accuracy.
For CNOs focused on readmission and care coordination metrics, better handoffs strengthen continuity across units and into post-acute settings.
Contrast manual recap with AI-supported clarity. One increases stress. The other builds confidence.
E. Real-Time Quality Measure Prompts for VBC Contracts
Value-based contracts reward precision.
Missing documentation can cost thousands in lost incentives. Nurses are often the frontline data stewards for measures tied to falls, pressure injuries, immunizations, and discharge education.
AI agents for nurses can flag missing quality elements before the chart closes.
Instead of retrospective audits, nursing AI agents provide:
- In-shift prompts for incomplete measures
- Evidence-based intervention reminders
- Automated tagging for quality reporting
This shifts quality from cleanup to prevention.
CIOs and CFOs care about predictable performance. CNOs care about fairness. Nurses should not carry financial risk because a field was buried three screens deep.
F. Capacity Management and Throughput Coordination
Throughput is a nursing issue.
Bed turnover delays, discharge bottlenecks, and transport coordination often fall to nurse leaders. AI agents for nurses can integrate with bed management systems and care coordination tools to:
- Identify discharge-ready patients earlier
- Flag barriers to placement
- Predict staffing pinch points
When AI-generated nursing documentation feeds real-time dashboards, operational leaders gain visibility without adding to the reporting burden.
A memo does not solve throughput. It is solved by workflow intelligence.
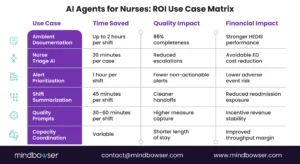
Table 1: Top 6 AI Agents for Nurses’ Use Cases
| Use Case | Time Savings | Quality Impact | VBC Alignment |
| Ambient Documentation | 2 hrs/shift | 95% completeness | HEDIS scores |
| Triage Decision Support | 30 min/case | Reduced escalations | Avoidable ED |
| Alert Prioritization | 1 hr/shift | Alarm fatigue ↓45% | Readmissions |
| Clinical Summarization | 45 min/shift | Handoff accuracy ↑ | Care coordination |
| Real-Time Quality Prompts | 30–60 min/shift | Measure capture ↑ | Incentive revenue |
| Capacity Coordination | Variable | Discharge delays ↓ | LOS reduction |
Notice the pattern. Every use case ties time savings to a quality or revenue metric.
AI agents for nurses are not chat tools. They are operational infrastructure. Built correctly, they reduce documentation burden, strengthen compliance, and improve throughput in the same motion.
And for CNOs under pressure to protect bedside time while hitting VBC targets, that alignment is the difference between pilot fatigue and platform strategy.
The ROI case is strongest when AI agents for nurses are embedded in real nurse workflows, not on top of them.
Ready to implement AI agents for nurses without workflow risk?
III. Governance, Integration, and EHR Reality: What Separates Real AI Agents for Nurses from Pilot Theater
Every CNO has seen it.
A slick demo. A fast pilot. A press release. Then six months later, low adoption, frustrated nurses, and compliance questions no one can answer.
AI agents for nurses only become operational assets when governance and EHR integration are designed from day one. Otherwise, they add risk instead of reducing burden.
This is where executive evaluation gets serious.
A. Governance First: Protect Licensure, Protect the Organization
Nursing leaders carry licensure risk. CMIOs carry clinical integrity risk. CIOs carry data security risk. No one wants an AI hallucination documented in a patient chart.
Regulatory scrutiny around AI in clinical workflows is increasing, especially when decision support influences care plans. That means AI agents for nurses must meet four core governance criteria:
- Traceability
Every recommendation, prompt, or structured entry must log source data and reasoning logic. - Human-in-the-Loop Validation
AI nursing documentation should require nurse confirmation before final submission to the EHR. - Audit-Ready Logs
Suppressed alerts, triage suggestions, and quality prompts must be reviewable during internal audits. - HIPAA + SOC 2 Architecture by Design
Not bolted on later. Encryption, access control, and role-based permissions must align with enterprise standards.
Short rule. No exceptions.
A governance-first approach reassures boards and frontline staff alike. Nurses need to trust that AI agents for nurses will not override their clinical judgment. CIOs need confidence that data flows remain secure and compliant.
Contrast shadow IT pilots with enterprise-grade deployment. One generates headlines. The other generates durability.
If your nursing AI agents cannot pass a compliance tabletop exercise, they are not ready for scale.
B. EHR Integration: The Make-or-Break Variable
Let’s be blunt.
If AI agents for nurses sit outside the EHR, adoption drops. Fast.
KLAS research consistently shows that deep EHR integration is a top predictor of sustained clinical AI use. Deep EHR integration is a top predictor of sustained clinical AI use. Tools that require context switching, duplicate logins, or manual reconciliation are associated with lower nurse satisfaction and higher abandonment rates.
For nursing AI agents, integration must include:
- Direct write-back to structured flowsheets
- Role-based contextual prompts
- Real-time data ingestion from vitals, labs, and orders
- Single sign-on and uptime above 99%
Anything less feels like extra work.
For technical leaders evaluating vendors, the question is not “Does it integrate?” The question is “At what layer?”
API-level integration that maps directly to your EHR schema supports durable AI nurse workflows. Screen-scraping or surface overlays introduce fragility.
The emotional factor matters too. Nurses do not want another screen. They want relief inside the screen they already use.
AI agents for nurses must operate invisibly within existing nurse workflows. That is the bar.
C. Build vs. Buy vs. Retrofit: Why Nursing Requires Custom Architecture
Here is the uncomfortable truth.
Many AI platforms began with physician documentation use cases and later extended into nursing. The workflows are not the same. The data structures are not the same. The risk models are not the same.
Nursing AI agents require:
- Flowsheet-specific logic
- Shift-based summarization
- Triage protocol mapping
- Quality-measure tagging aligned to VBC contracts
A one-size approach rarely holds.
This is where a custom-build strategy matters. When AI agents for nurses are architected around your specific:
- EHR configuration
- Quality contracts
- Staffing model
- Care setting
You avoid brittle retrofits and costly rework.
At Mindbowser, for example, AI accelerators are designed to launch about 40% faster while still allowing full customization and client-owned IP. That balance of speed and specificity is what CNOs need. Fast results. No lock-in.
This works. Period.
Table 2: AI Nursing Evaluation Scorecard
Before expanding pilots, many systems use a 30-day scorecard to validate operational fit.
| Criterion | Weight | Week 4 Target |
| Documentation Time | 30% | >25% reduction |
| Flowsheet Accuracy | 25% | >95% completeness |
| Nurse Satisfaction | 20% | NPS lift >15 pts |
| Safety Incidents | 15% | Zero hallucinations |
| Integration Uptime | 10% | >99% |
Notice what is absent. Vanity metrics.
This scorecard ties AI agents for nurses directly to documentation burden, safety, satisfaction, and uptime. If a pilot cannot hit these benchmarks within four weeks, scaling becomes harder to justify.
So what separates durable nursing AI agents from pilot theater?
Three things:
Governance.
Deep EHR integration.
Workflow-native architecture.
Miss any one of those, and adoption stalls.
Get them right, and AI agents for nurses become part of your operating system, not a temporary experiment.
For CNOs and CMIOs, the evaluation lens must shift from “Does it sound smart?” to “Does it integrate, comply, and measurably reduce burden within 30 days?”
Because bedside time is too valuable for half-measures.
IV. From Pilot to Platform: How to Deploy AI Agents for Nurses in 30 Days Without Disrupting Care
You do not need a 12-month transformation plan.
You need a controlled, measurable, governance-first rollout that proves AI agents for nurses can reduce documentation burden, improve throughput, and protect bedside time within 30 days.
That is the difference between innovation theater and operational impact.
Here is how leading CNOs and CIOs are doing it.
A. Start with One High-Impact Workflow, Not the Entire Nursing Stack
Scope creep kills momentum.
The most successful deployments of nursing AI agents begin with a single workflow where documentation burden is high, and metrics are visible. In most organizations, that means:
- Ambient AI nurses for med-surg documentation
- ED or call-center nurse triage AI
- Shift handoff summarization in high-acuity units
Why start narrow?
Because it allows clean measurement of:
- Documentation time reduction
- Flowsheet completeness
- Nurse satisfaction
- Quality measure capture
If you try to roll out AI nurse workflows across every unit simultaneously, variance clouds the data, and resistance grows.
One workflow. One metric set. One month. That discipline builds credibility fast.
Prove time savings and safety in one area before scaling systemwide.
B. Build the 30-Day Pilot Around Operational Metrics, Not Technical Features
Nurses do not care about model architecture. They care about whether charting ends on time.
Your 30-day roadmap should include four phases:
Week 1: Governance and Integration Validation
- Confirm HIPAA and SOC 2 controls
- Validate EHR write-back to structured fields
- Run compliance tabletop scenario
Week 2: Limited Unit Rollout
- 10 to 25 nurses
- Real patient encounters
- Human-in-the-loop validation active
Week 3: Data Review and Adjustment
- Measure documentation time per shift
- Track flowsheet completeness
- Review alert suppression logs
Week 4: Executive Review
- Compare against scorecard targets
- Conduct a nurse NPS survey
- Identify expansion path
Short cycles win trust.
During ambient AI pilots cited in industry reports, documentation time dropped significantly while completeness improved when AI nursing documentation was written directly to flowsheets instead of narrative-only notes.
This is the critical insight. AI agents for nurses must reduce clicks, not add them.
When week four shows:
- 25% documentation time reduction
- 95% flowsheet completeness
- Zero safety incidents
- Uptime above 99%
You have an expansion case that speaks CFO language.
C. Tie AI Agents for Nurses Directly to Retention and VBC Revenue
Here is the executive lens.
If your system employs 500 bedside nurses and ambient AI nurses save 90 minutes per shift on average, the reclaimed time amounts to thousands of hours per month. Even if only half translates into reduced overtime or improved throughput, the financial return compounds quickly.
But the deeper value is retention.
Becker’s reports ongoing concerns about nurse burnout and turnover across hospital systems. If AI agents for nurses reduce after-shift charting and cognitive overload, retention curves can shift. Even a 5% improvement in retention can offset significant recruitment and onboarding costs.
Then layer in VBC.
When AI nursing documentation captures quality elements accurately in real time, missed incentives decrease. HEDIS performance stabilizes. Readmission penalties drop. Care coordination improves.
The value chain looks like this:
Documentation time ↓
Burnout ↓
Retention ↑
Quality capture ↑
VBC revenue stability ↑
Three levers. One platform.
This works. Period.
D. Architect for Scale Without Losing Nursing Specificity
After a successful pilot, expansion should follow a controlled pattern:
- Extend to adjacent units with similar workflows
- Maintain governance oversight through quarterly reviews
- Continuously retrain models based on nurse feedback
- Align AI nurse workflows with evolving VBC contract requirements
This is not a one-time deployment. It is an evolving capability.
The mistake many systems make is freezing the configuration after initial rollout. Nursing practice evolves. Quality measures change. AI agents for nurses must adapt without compromising auditability.
That requires:
- Version control of prompts and logic
- Transparent model updates
- Structured nurse feedback loops
Contrast static deployment with living infrastructure. One stagnates the other compounds value.
E. The Executive Decision Framework
Before scaling nursing AI agents, CNOs and CIOs should answer five questions:
- Does the solution write directly to structured EHR fields?
- Are all AI recommendations traceable and auditable?
- Has documentation time dropped by at least 25%?
- Has nurse satisfaction measurably improved?
- Can we tie outcomes to retention or VBC performance?
If the answer is yes across the board, you are not experimenting. You are building operational advantage.
If not, refine before expansion.
The New Standard for Nursing Operations
The conversation has shifted.
It is no longer “Should we explore AI?” It is “Which AI agents for nurses can safely and measurably reduce burden within our existing EHR environment?”
Nursing leaders sit at the intersection of care quality, workforce stability, and financial performance. Few technologies influence all three at once. Properly designed AI agents for nurses do.
They turn ambient conversations into structured data.
They turn alerts into prioritized action.
They turn documentation from after-hours stress into in-shift efficiency.
And most importantly, they protect bedside time.
That is the metric that matters.
AI agents for nurses are built specifically for nursing workflows, not adapted from physician documentation tools. They write directly to structured EHR flowsheets, support real-time triage and alert prioritization, and align with nursing shift patterns. The focus is on reducing the documentation burden while improving the capture of quality, not just on generating narrative notes.
In well-designed deployments, AI agents for nurses can reclaim up to two hours per shift through ambient documentation and workflow automation. Most organizations target at least a 25% reduction in documentation time within the first 30 days of a controlled pilot.
Not when designed with governance first. Effective nursing AI agents include human-in-the-loop validation, audit logs, traceable recommendations, and HIPAA and SOC 2-aligned architecture. Nurses maintain final clinical authority, and all AI-supported entries are reviewable.
By reducing after-shift charting and the cognitive overload caused by alerts and manual documentation, AI agents for nurses can lower frustration and improve job satisfaction. Even modest improvements in retention can offset significant recruitment and onboarding costs for health systems.
Start with a focused 30-day pilot tied to operational metrics: documentation time reduction, flowsheet completeness above 95%, zero safety incidents, improved nurse satisfaction, and EHR uptime above 99%. If those benchmarks are met, expansion becomes a strategic decision rather than a technology experiment.