



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
Standardized chronic care management templates reduce documentation errors, improve compliance, and speed enrollment while ensuring measurable ROI. Hospitals and digital health leaders who use structured templates experience stronger audit readiness and revenue capture.
Managing patients with multiple chronic conditions requires precision and care. Every missed signature, incomplete time log, or vague care plan note creates risk, risk of failed audits, denied claims, or worse, patients falling through the cracks. For hospitals and digital health programs, the absence of standardized templates translates into wasted staff hours, inconsistent documentation, and lost revenue opportunities.
The answer is not another binder of forms. What providers need is a set of purpose-built chronic care management templates that align with Medicare and Medicaid requirements, fit seamlessly into EHR workflows, and make compliance the default rather than an afterthought. When enrollment, care plans, and monthly documentation are structured and standardized, organizations see immediate gains in both efficiency and quality.
The deepest single-template asset in this set is the printable CCM care plan template, a downloadable PDF and Word version, with a fully filled-in patient example, that satisfies CMS documentation requirements out of the box. Most of the templates introduced below are extensions of that core care plan; the link covers what the rest of this page references.
This guide breaks down the essential CCM templates your organization should use in 2026, from enrollment and consent forms to compliance and audit-ready documentation. We will also explore how digital intake outperforms manual approaches and provide a complimentary CCM Template Pack that your teams can adapt immediately.
The insights presented here are designed for mid-market hospitals, FQHCs, RHCs, and growth-stage digital health startups that aim to scale their CCM programs without compromising compliance or revenue.
This guide focuses on the operational template set: enrollment, consent, monthly documentation, compliance, and audit forms- that a CCM program needs to run cleanly day-to-day. If you’re looking for the technical architecture behind the care plan specifically (FHIR CarePlan resources, US Core format, EHR integration patterns for Epic and Cerner), the printable CCM care plan template is the deeper companion to this page. That page also includes a fully filled-in care plan for a different patient (Mrs. Margaret Johnson, 72, with diabetes, heart failure, and hypertension); useful as a second worked example alongside Mrs. Thompson below.
I. Why Templates Matter For CCM Outcomes and ROI
A. Administrative Burden and Compliance Risk
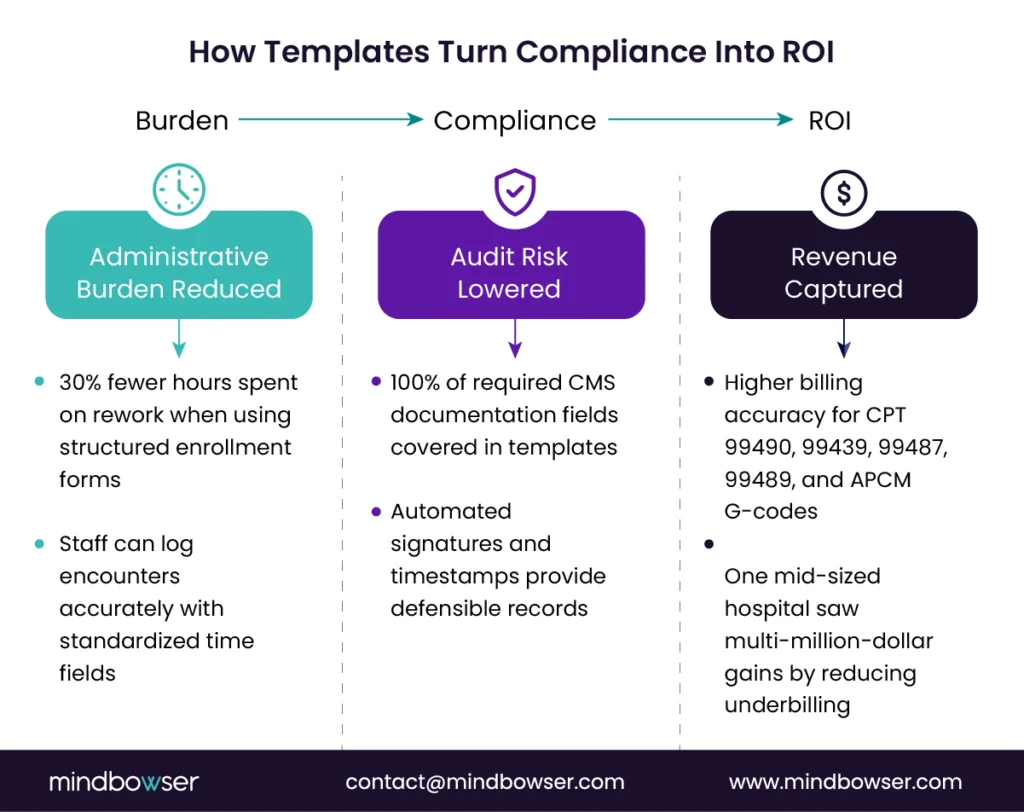
- Time lost to rework and missing fields
CCM teams often spend hours chasing down missing patient consent forms, incomplete care plans, or incorrect time logs. A nurse may complete a call, but without a standardized field for capturing total time or staff role, the encounter becomes non-billable. This repetitive rework not only drains staff productivity but also erodes trust in the program. - Audit exposure from inconsistent documentation
Medicare and Medicaid auditors closely scrutinize CCM documentation. A full breakdown is covered in our CCM care plan requirements guide. Inconsistent formats, vague notes, or missing attestations can trigger clawbacks and financial penalties. Templates enforce uniformity by ensuring that every care plan, consent form, and monthly summary meets regulatory expectations. A structured template also provides an audit-ready trail with timestamps, signatures, and code-specific evidence. - Revenue impact across multiple programs
Chronic care management overlaps with other care coordination programs, including remote patient monitoring (RPM), Principal Care Management (PCM), and the new Accountable Care Management (APCM) codes. Without standardized templates, providers risk underbilling or failing to capture all eligible services. Every missed code translates into lost revenue, and at scale, the leakage can amount to millions of dollars annually for a mid-sized hospital system.
B. Standardization That Improves Quality
- Consistent consent, care plans, and summaries
Templates eliminate guesswork. Whether the patient is enrolled in CCM at a rural health clinic or a hospital outpatient department, the intake process looks the same. Consent language is uniform, care plans follow a consistent structure, and summaries include all required elements. This consistency fosters reliability across teams and sites, thereby reducing errors and enhancing the patient experience. - Equity by design
Well-designed templates incorporate plain language, reading-level adjustments, and translation into multiple languages. By making enrollment forms and care plans easier to understand, providers can better engage patients with limited literacy or English proficiency. Equity is no longer an afterthought but is baked into the structure of the documentation. - Built-in clinical prompts
Care plans are not static documents. Templates can embed prompts and reminders that guide care managers to address recommended screenings, preventive measures, or guideline-based interventions. These clinical nudges enhance adherence to evidence-based protocols, which in turn lead to improved patient outcomes and stronger quality measure reporting.
When teams need a starting point rather than a from-scratch build, the printable CCM care plan template provides a CMS-compliant baseline that can be adopted as-is or used as the structural reference for a custom EHR-embedded version.
Related read – Headless EHR Comparison: Medplum vs Healthie vs OpenEMR vs Oystehr vs Canvas
C. Data Interoperability And EHR Fit
- Mapping to FHIR/HL7 standards
A chronic care management template should not exist in isolation. By mapping fields to FHIR CarePlan, Condition, and observation resources, templates integrate seamlessly into major EHR systems like Epic, Cerner, Meditech, Athena, Healthie, and Canvas. This ensures that data entered once can flow across systems without duplication or manual re-entry. - Time logging and task evidence
Accurate time capture is essential for billing CCM and APCM codes such as CPT 99490, 99439, 99487, 99489, and G-codes for complex care management. Templates can structure these logs by staff role, task category, and duration, creating clear evidence that supports coding and billing. This reduces claim denials and strengthens financial performance. - Reporting fields for ROI and audits
Templates that include standardized reporting fields enable organizations to track enrollment rates, call completion rates, intervention effectiveness, and revenue capture. They also produce a clear record for payer audits, ensuring that a complete and compliant documentation trail backs every billed claim. In value-based care contracts, this data becomes essential for proving quality and cost outcomes.
Related read: Chronic Care Management Billing in 2026: From CPT Codes to APCM Strategy
II. The Core Chronic Care Management Template Set
A. Enrollment and Consent Templates
- Medicare-compliant consent language and revocation notices
CMS requires explicit patient consent before enrollment in CCM. Without a standardized form, care teams risk missing critical language or failing to document revocation rights. Templates ensure that every patient is informed about service scope, potential cost-sharing, and the option to withdraw at any time. This protects both the patient and the provider from future disputes. - Medicaid and state-specific variants
Medicaid programs vary significantly across states, and FQHCs or RHCs often operate under additional layers of compliance. A core CCM template must be adaptable to reflect state policy requirements. For example, some states require additional disclosures around managed care organizations or specify unique billing language. Standardized variants reduce confusion and streamline enrollment across different payer contracts. - Identity, eligibility, and attribution fields
Beyond the consent signature, a strong enrollment template captures patient identifiers, payer details, and attribution to a primary care provider. These fields prevent eligibility errors and ensure that billing aligns with the correct provider of record. When integrated with EHR or payer feeds, these templates reduce enrollment errors that lead to claim denials.
B. Care Plan and Monthly Documentation Templates
- Structured problem list and interventions
A chronic care management template should guide care managers through a structured workflow that includes a problem list, patient-centered goals, identified barriers, planned interventions, and scheduled follow-ups. By mapping these fields to FHIR CarePlan objects, the template ensures interoperability with EHR systems. This structured approach creates consistency across providers while making care plans actionable. - Time capture and staff role tracking
Monthly CCM encounters are billable only when time thresholds are met. Templates that include fields for total minutes, staff credentials, and task categories eliminate ambiguity. Whether documenting a 20-minute 99490 encounter or a 60-minute 99487 complex visit, staff can log activity in real time with evidence tied directly to the code billed. - Social determinants of health (SDOH) capture
Health outcomes often hinge on factors outside clinical care. Modern CCM templates include standardized SDOH screening questions, referral tracking, and resolution fields. By embedding tools such as PRAPARE or state-approved screening tools, providers can systematically identify and address non-clinical barriers, thereby closing referral loops. This not only improves patient outcomes but also supports value-based care reporting.
To see how this translates into practice, review a CCM care plan example with completed goals, interventions, and timelines.
C. Compliance and Audit Templates
- HIPAA, SOC 2, and 42 CFR Part 2 checklists
Every CCM workflow must meet federal and state privacy requirements. Templates that embed checklists aligned with HIPAA, SOC 2, and 42 CFR Part 2 regulations provide staff with guardrails for compliance. This includes ensuring consent to share sensitive health information and properly managing patient communication preferences. - Audit trail and versioning
Audit readiness encompasses more than just complete documentation. Templates that automatically include timestamps, digital signatures, and version history create defensible records. If a payer review occurs, the organization can quickly demonstrate compliance by producing standardized, verifiable documentation. - Billing artifacts for RHCs and FQHCs
Rural health clinics and federally qualified health centers face unique billing challenges. Templates can include dedicated sections for capturing encounter justification, exception notes, and supporting documents. This provides an added layer of protection against claim rejection and ensures that clinic staff does not have to reinvent processes for every payer audit.
The templates below are ready to use. Adapt them to your EHR workflows, state-specific Medicaid rules, or APCM transition. PDF for print, Word for editing.
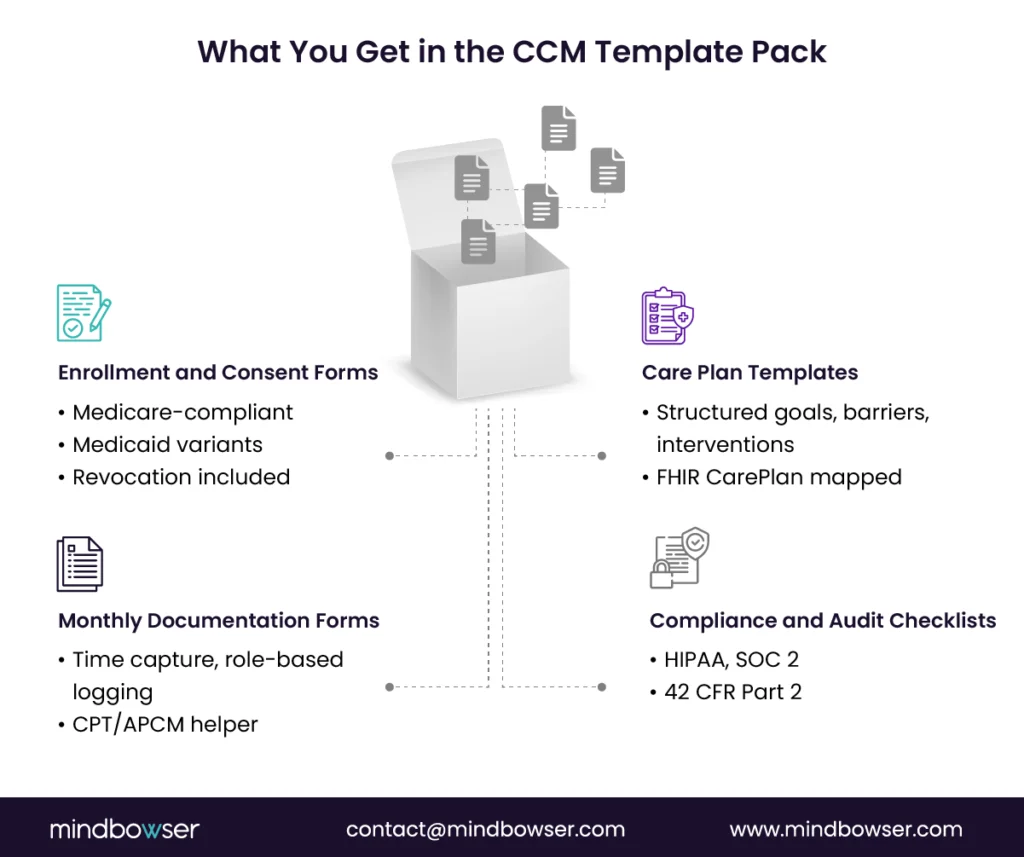
What’s included in the CCM Template Pack:
- Medicare CCM Enrollment Form (patient-facing, plain language)
- Patient Consent Form (includes verbal + written consent options)
- Monthly Care Plan Template (7 CMS-required elements pre-filled)
- Monthly Documentation Template (time tracking + care coordinator notes)
- Compliance Checklist (HIPAA, SOC 2, audit artifact list)
Get the Documentation Toolkit You Need to Stay Audit-Ready and Compliant
Discover how Mindbowser’s digital workflows and interoperability tools can help your team improve efficiency and compliance.
III. What These Templates Look Like Filled In: A Sample Patient Walkthrough
A blank template framework is half the picture. The other half is showing what the templates look like for a real CCM patient, what fields get filled, what level of detail auditors expect, how enrollment, consent, and the care plan stitch together into one defensible documentation pack. Below is a sample patient running through both an enrollment form and a care plan. Names and identifiers are illustrative; the structure matches the template categories described above and meets CMS Chronic Care Management documentation requirements.
Note for readers who landed here from the printable CCM care plan template page: that page features a different patient (Mrs. Margaret Johnson, 72, with diabetes, heart failure, and hypertension). This page covers Mrs. Patricia Thompson (78, with atrial fibrillation, osteoarthritis, and depression). Two different patients, two different sets of comorbidities; same template framework. Pick whichever profile is closer to your typical CCM patient as your reference.
Patient Snapshot
| Field | Entry |
| Patient | Patricia Thompson (Mrs. Thompson) |
| Age / Sex | 78 / Female |
| MRN | 008-552-1837 (sample) |
| Primary Insurance | Medicare Part B + Medigap Plan F |
| Living Situation | Lives alone in single-family home; widowed (2022) |
| Functional Status | Independent in ADLs; mild limitations with stairs and prolonged walking |
| CCM Enrollment Date | 2026-01-15 |
| Care Coordinator | Jennifer L., RN (assigned 2026-01-22) |
Sample 1: CCM Enrollment Form (filled in)
Form section A: Patient Demographics + Insurance Verification
| Field | Entry |
| Full Legal Name | Patricia Anne Thompson |
| DOB | 1947-11-04 |
| Address (Verified) | (sample address on file) |
| Primary Phone | (sample) |
| Best Contact Time | Mornings, 9 AM – 12 PM |
| Emergency Contact | Daughter, Linda Thompson-Reyes (sample contact) |
| Medicare Number | (verified, on file) |
| Medicare Part B Effective Date | 2012-12-01 |
| Secondary Insurance | Medigap Plan F (verified active) |
| Cost-Share Status | Medigap covers 20% Part B coinsurance: patient out-of-pocket: $0/month for CCM |
Form section B: CCM Eligibility Verification
| Eligibility Criterion | Status | Documentation |
| Has 2+ chronic conditions expected ≥12 months | ✅ Confirmed (3 conditions documented) | Problem list verified against EHR |
| Conditions place patient at significant risk | ✅ Confirmed | AFib stroke risk + MDD relapse risk + OA functional decline |
| Initiating visit completed | ✅ Annual Wellness Visit (AWV) | 2026-01-08 with Dr. Anna Patel, MD |
| Patient not enrolled in CCM with another practitioner this month | ✅ Confirmed | Verified via insurance check |
Form section C: Active Problem List (with ICD-10)
| Condition | ICD-10 | Onset | Severity / Status |
| Paroxysmal Atrial Fibrillation | I48.0 | 2021 | On apixaban 5mg BID; stable, last episode 2025-09 |
| Bilateral Primary Osteoarthritis of Knees | M17.0 | 2019 | Pain 7/10 with prolonged activity; impacts ambulation |
| Major Depressive Disorder, recurrent, moderate | F33.1 | 2022 (post-bereavement onset) | PHQ-9 score 14 at intake (2026-01-15); on sertraline 100mg daily |
Form section D: Patient Consent
| Consent Element | Captured | Method |
| Patient acknowledges enrollment in CCM | ✅ | Verbal consent, witnessed by Jennifer L., RN |
| Patient understands cost-share (or supplemental coverage) | ✅ | Medigap covers 20%: confirmed with patient |
| Patient understands right to revoke consent at any time | ✅ | Acknowledged verbally |
| Patient consents to electronic care plan storage and sharing | ✅ | Acknowledged verbally |
| Date of Consent | 2026-01-15 | Documented in EHR encounter note |
| Practitioner of Record | Dr. Anna Patel, MD | Listed on consent record |
Form section E: Communication Preferences
| Preference | Selection |
| Preferred Contact Method | Phone call (patient declined SMS) |
| Patient Portal Access | Active (uses patient portal weekly with help from daughter) |
| Authorized to Discuss with Family | Yes: daughter Linda Thompson-Reyes (HIPAA authorization on file) |
| Language Preference | English |
| Hearing/Vision Accommodations | Mild hearing loss in right ear; speak clearly on left side |
Form section F: 24/7 Access Protocol Acknowledgment
| Element | Status |
| Patient given practice 24/7 line | ✅ Card provided 2026-01-15 |
| After-hours protocol explained | ✅ Practitioner-on-call coverage explained |
| Patient understands when to call vs go to ED | ✅ Verbal teach-back confirmed |
Form section G: Initial Care Coordinator Assignment
| Element | Entry |
| Assigned Care Coordinator | Jennifer L., RN |
| Backup Coordinator (for vacation/coverage) | Marcus T., RN |
| First Scheduled Outreach Call | 2026-02-01 (planned) |
| Coordinator Caseload at Assignment | 248 patients (within target range) |
Audit-ready check: Every required CCM enrollment element captured with date, witness/practitioner, and method. The form is structured EHR data, not a free-text note or scanned upload.
Sample 2: Care Plan (filled in for the same patient)
Section A: Care Plan Header
| Field | Entry |
| Care Plan Version | v1.0: initial (2026-01-22) |
| Last Reviewed | 2026-04-15 (Q1 review) |
| Next Scheduled Review | 2026-07-15 (Q2 review) |
| Plan Author | Jennifer L., RN |
| Plan Approver | Dr. Anna Patel, MD (signed off 2026-01-25) |
| Distribution | Patient (printed copy 2026-01-22), daughter (patient portal 2026-01-22), Dr. Patel (EHR notification 2026-01-22), care team (EHR shared) |
Section B: SMART Care Plan Goals
Goal 1: AFib stroke prevention and rhythm control
Maintain therapeutic anticoagulation (apixaban adherence ≥ 90% by pharmacy fill data) and zero AFib-related ED visits or hospitalizations over the next 12 months. Target reassessment: monthly adherence check, quarterly cardiology review.
Goal 2: Pain management and functional independence
Reduce average daily knee pain from 7/10 to ≤ 4/10 within 90 days through PT, weight management, and medication optimization. Maintain ability to climb 10 stairs and walk 1 block independently. Target reassessment: 2026-04-15 (90-day pain reassessment).
Goal 3: Depression management and social engagement
Reduce PHQ-9 score from 14 (moderate depression) to < 10 (mild) within 6 months through medication adherence (sertraline ≥ 90% adherence), bi-weekly RN check-ins, and re-engagement with at least one weekly social activity. Target reassessment: 2026-07-15 (6-month PHQ-9 retest).
Goal 4: Fall prevention and home safety
Reduce fall risk by completing in-home safety assessment within 60 days, addressing identified hazards, and maintaining lower-extremity strength via PT. Goal: zero falls in 12 months. Target reassessment: 60-day post-PT-completion check.
Section C: Planned Interventions
| Intervention | Frequency | Owner | Documentation |
| RN care coordination call | Bi-weekly (twice monthly) | Jennifer L., RN | EHR call note + minutes log |
| PHQ-9 administration | Monthly x 3, then quarterly | Jennifer L., RN | Structured PHQ-9 tool in EHR |
| Home pulse + rhythm log review (BP captured opportunistically) | Weekly (patient logs daily; RN reviews weekly) | Jennifer L., RN | RPM dashboard with rhythm-strip review, AFib episodes flagged |
| Pharmacist medication review (incl. apixaban + sertraline interaction monitoring) | Quarterly | David K., PharmD | Med rec note + adherence summary + interaction surveillance |
| PCP visit | Quarterly (scheduled) | Dr. Anna Patel, MD | EHR encounter note |
| Cardiology follow-up | Every 6 months | Dr. Mark Chen, Cardiology | Specialist note + AFib status review |
| Orthopedic / PT consult + therapy | PT 2x/week x 8 weeks, then maintenance | PT clinic | Structured PT progress notes |
| Behavioral health follow-up | Every 4-6 weeks (telehealth acceptable) | Dr. Sarah Reyes, LCSW | Therapy session notes |
| In-home safety assessment | One-time within 60 days of enrollment | Home health OT | Safety assessment report + recommendations |
| SDOH screening | At enrollment + every 6 months | Jennifer L., RN | Structured SDOH note in EHR |
Section D: Care Team
| Role | Name | Contact | Responsibility |
| Primary Care Physician | Dr. Anna Patel, MD | (sample) ext. 4421 | Clinical decisions, plan approval, quarterly visit |
| Care Coordinator (RN) | Jennifer L., RN | (sample) ext. 4422 | Bi-weekly outreach, RPM monitoring, plan execution |
| Cardiology | Dr. Mark Chen, MD | (sample) | AFib management, anticoagulation oversight |
| Behavioral Health | Dr. Sarah Reyes, LCSW | (sample) | Depression management, weekly therapy |
| Clinical Pharmacist | David K., PharmD | (sample) ext. 4423 | Quarterly med review, polypharmacy check |
| Physical Therapist | (sample PT clinic contact) | (sample) | Knee OA rehabilitation |
| Occupational Therapist (home safety) | (sample home health agency) | (sample) | One-time home safety assessment |
| Patient | Mrs. Thompson | (patient phone) | Daily monitoring, adherence, reporting symptoms |
| Authorized Family Contact | Linda Thompson-Reyes (daughter) | (sample) | Plan visibility, escalation contact |
Section E: Follow-Up Schedule (first 6 months)
| Month | Touchpoints | Goals Reviewed |
| Month 1 (Jan 2026) | Enrollment, initial RN call, PT start, RPM setup, first PHQ-9 | All 4 goals: establish baseline |
| Month 2 (Feb 2026) | 2 RN calls, second PHQ-9, in-home safety assessment, cardiology check-in | Goal 3 (PHQ-9 trend), Goal 4 (safety) |
| Month 3 (Apr 2026) | 2 RN calls, third PHQ-9, PT progress check, PCP quarterly visit | All 4 goals: Q1 review and plan v2 |
| Month 4–5 | Bi-weekly RN calls, PT maintenance phase, behavioral health continued | Goals 1–4 progress check |
| Month 6 (Jul 2026) | Full plan review, 6-month PHQ-9, full goal reassessment, plan version update to v3.0 | All 4 goals: major reassessment |
Section F: SDOH and Barriers
| Domain | Status | Action |
| Transportation | At risk: patient relies on daughter or paratransit for medical appointments | Coordinated with daughter for PCP/cardiology visits; paratransit referral for PT 2x/week |
| Social Isolation | Significant: widowed 2022, lives alone, contributing factor to MDD | Referred to senior center 2 days/week; daughter visits 2x/week; weekly RN check-in maintained |
| Food Security | Stable | No action |
| Medication Affordability | Stable on Medigap | Pharmacist monitors quarterly for cost concerns |
| Home Safety | Pending assessment | OT scheduled within 60 days; preliminary report on bathroom grab bars + stair rail |
| Caregiver Support | Daughter actively involved | Daughter included in care plan signature and quarterly updates |
| Hearing Accommodation | Mild right-ear hearing loss | All RN calls noted to speak on left side; in-person visits use written summary backup |
Section G: Audit-Readiness Notes
This care plan + enrollment pack would withstand an OIG audit because:
1. Eligibility is explicit: three qualifying chronic conditions with ICD-10 codes, severity, and onset dates
2. Consent is complete: date, method (verbal), witness (RN), practitioner (MD), revocation rights acknowledged, cost-share disclosed
3. Initiating visit is documented: AWV with Dr. Patel on 2026-01-08, encounter note linked
4. Care plan is structured EHR data: not a Word document, not a PDF upload
5. Goals are SMART: measurable, time-bound, with reassessment dates
6. Every intervention has an owner and a frequency: auditors look for this; missing owners are the most common gap
7. Plan versioning is visible: v1.0 → planned v2.0 → v3.0
8. Distribution history is logged: date, recipient, method for each
9. Time logs (when added monthly) tie back to specific care plan elements: every billable minute traces to a planned intervention
10. SDOH is structured, not narrative: domain-by-domain, with status and action
This is the documentation discipline that separates a CCM program that bills cleanly from one that gets clawed back. The forms above aren’t more elaborate than a typical EHR can support: they’re just used disciplinedly.
Build A Scalable, Audit-Ready CCM Program
Discover how Mindbowser’s digital workflows and interoperability tools can help your team improve efficiency and compliance.
IV. Digital Intake Versus Manual: What To Choose and When
A. Digital Intake Advantages
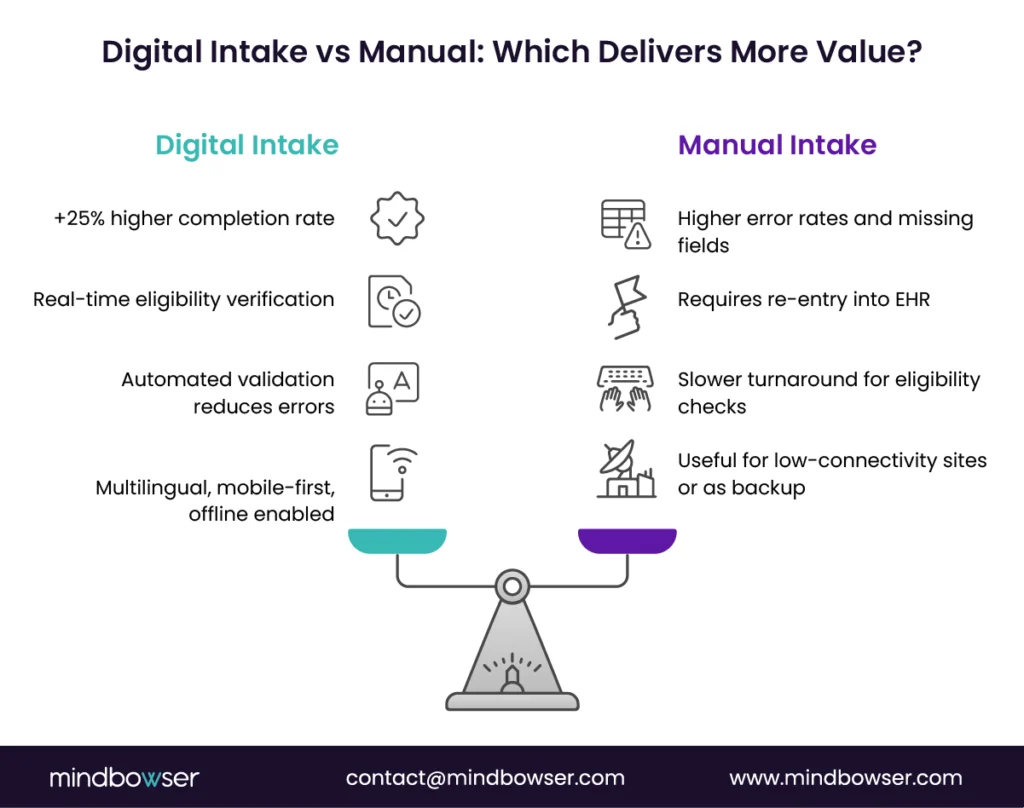
- Higher completion and fewer errors
Digital templates reduce incomplete or inaccurate information by guiding patients and staff through structured fields, ensuring accurate data collection. Automated validations flag missing signatures, incomplete time entries, or inconsistent payer details before submission. Hospitals that transitioned from paper-based intake to digital platforms have reported a rise in completion rates of more than 25%, accompanied by a corresponding decrease in claim rejections. - Real-time eligibility and financial assistance
Digital intake connects enrollment forms directly to payer databases and financial assistance modules, streamlining the process for both patients and healthcare providers. Eligibility can be verified instantly, ensuring patients qualify for CCM services before care begins. Some organizations also embed automated financial triggers that flag patients who may be eligible for Medicaid redetermination or charity care programs. This prevents enrollment errors and helps reduce bad debt. - Accessibility at scale
Patients are more likely to complete the intake process when it meets them where they are, rather than requiring them to adapt to a specific process. Mobile-first templates, multilingual options, and plain-language prompts improve accessibility for older adults, low-literacy populations, and non-English speakers. Offline functionality allows field staff to collect data during home visits, which later syncs seamlessly into the EHR. Digital intake reduces disparities by addressing access barriers from the start.
B. When Manual Templates Still Fit
- Low-connectivity or resource-limited sites
Not every care setting has stable broadband or digital infrastructure. Community clinics and rural practices may need to rely on paper forms as a temporary solution. In these cases, manual templates offer a structured approach to collecting essential data until connectivity improves or digital systems are implemented. - Workarounds during EHR transitions
Hospitals undergoing an EHR migration often face gaps where digital workflows are disrupted. Manual templates act as a fallback, ensuring CCM documentation continues without risking compliance or billing delays. These paper-based workflows can later be digitized and uploaded into the new system. - Hybrid workflows
Some organizations maintain a blend of manual and digital templates. For example, patients may complete a paper intake during a home visit, but staff use scanning and optical character recognition tools to convert it into structured fields. Hybrid workflows preserve the patient experience while supporting downstream digital reporting.
C. Implementation Playbook
- Build-buy-partner decisions
Organizations must weigh whether to develop digital templates in-house, purchase a solution, or partner with a vendor to meet their needs. In-house builds allow for customization but require a significant amount of IT bandwidth. Vendor solutions provide speed and regulatory updates, while partnerships with digital health companies can integrate templates directly into broader CCM platforms. - EHR integration patterns
For digital templates to succeed, they must connect with the EHR environment. Common approaches include SMART-on-FHIR apps, HL7 interfaces, or API-based integration. Choosing the right path depends on the hospital’s core system. Epic, Cerner, and Meditech often use HL7 or FHIR, while startups on Athena or Canvas can rely more heavily on APIs. - Change management and staff readiness
Even the best templates fail without staff adoption. Training programs that use a train-the-trainer model ensure that frontline staff are comfortable with new workflows. QA audits conducted within the first 90 days can catch issues before they become systemic, and a structured go-live checklist minimizes disruption. Leadership should communicate that templates are not “extra paperwork” but a tool to make billing, compliance, and patient care easier.
V. How Mindbowser Can Help
A. Ready-To-Use Workflows
ConnectHealth enables seamless data exchange between EHR systems and payer platforms, captures remote patient monitoring data and aligns it with CCM billing, and brings in vital-sign data from 300+ devices to enrich care plans with real-world health insights.
B. Case Study Proof Points
The pattern repeats across CCM-adjacent builds: when enrollment, consent, and care plan templates run as structured EHR data instead of Word documents, the operational metrics shift quickly. Three deployment patterns I’ve seen repeatedly:
Care coordination platform for an elderly chronic-care population
A custom-built care coordination platform deployed for a digital health company serving elderly Medicare patients embedded enrollment, consent, and care plan templates directly into the EHR rather than running them as separate intake systems.
Outcomes:
- 90% of enrolled patients engaged with the care management platform monthly
- Twice the report-generation speed of the prior manual system
- A small care team manages a larger panel without staffing increases
Workflow-automated chronic care platform on Epic
A chronic care platform built on top of an existing Epic deployment integrated wearable data, lab results, and AI-generated care plan drafts into a unified dashboard. The brief explicitly named documentation burden as the problem to solve.
Outcomes:
- 60% reduction in post-visit follow-up time
- 70% reduction in documentation time per patient
- 45% increase in monthly patient interactions
- Care plan generation moved from manual drafting to edit-and-approve workflow
SDOH-integrated population health platform
A platform built for a population health initiative integrated structured SDOH screening (PRAPARE-aligned), patient-reported outcomes, and clinician dashboards. Deployed across multiple state Medicaid populations with high social risk.
Outcomes:
- 67% reduction in emergency department visits among patients with documented social risk
- More timely intervention on transportation, housing, and medication affordability barriers
- SDOH data flowing directly into care plan goals and interventions, rather than living as separate notes
What These Have in Common
Every program with strong outcomes treated templates as live data structures, not as documents. The enrollment form, the consent record, the care plan, all sitting as structured EHR data that the workflow could query, validate, and update without manual transcription. That’s the architectural decision that makes the metrics move. The template content matters; the template format (structured data vs document) matters more.
C. Delivery and Compliance
Mindbowser’s delivery model is designed for scale and audit readiness. We integrate directly with leading EHR platforms, including Epic, Cerner, Meditech, Athena, Healthie, and Canvas. Every template and workflow aligns with HIPAA, SOC 2, and 42 CFR Part 2 requirements, ensuring privacy and compliance at every step.
For Medicaid programs, we provide support with contracting, payer packet preparation, and ROI calculators. This helps hospitals and health centers position their CCM programs not only as compliant but also as financially sustainable under both fee-for-service and value-based care models.
Conclusion
Templates are the backbone of a sustainable chronic care management program. Without them, hospitals and digital health teams risk inconsistent documentation, audit exposure, and missed revenue. With them, enrollment becomes faster, care plans are standardized, and compliance is embedded into daily workflows.
The key takeaway for 2026 is clear: organizations that standardize, digitize, integrate, and measure will be positioned to deliver higher-quality care while protecting their financial performance. Structured templates are no longer optional but essential for scaling CCM programs in both fee-for-service and value-based care models.
A chronic care management template is a structured form or digital workflow that captures all required documentation for Medicare, Medicaid, and commercial payer compliance. It covers patient consent, care plans, time logs, and monthly activity records. Templates ensure consistency across teams, reduce administrative burden, and provide audit-ready documentation for CCM and APCM programs.
CMS does not mandate a single standardized template, but it sets strict documentation requirements for consent, time capture, and care planning. Templates provide a consistent way to meet these requirements. Auditors often look for completeness, clarity, and alignment with billing codes, which makes standardized templates a practical necessity.
Paper templates can be effective in low-resource or rural settings, but they also increase the risk of incomplete or lost information. Digital templates offer real-time validation, EHR integration, and higher completion rates. The choice depends on infrastructure, but organizations moving toward digital intake see fewer claim denials and faster billing cycles.
The new Accountable Care Management (APCM) codes require more detailed documentation of complexity tiers, social determinants of health, and outcomes tracking. Templates adapted for APCM include additional fields for risk factors, referral tracking, and longitudinal outcomes. This ensures compliance with the evolving reimbursement models while supporting value-based care contracts.
The return on investment from templates can be measured through concrete metrics: enrollment rates, time-to-bill, denial rates, and per-patient margin. Hospitals that use standardized templates often report reduced rework, fewer audit findings, and a measurable increase in revenue capture from both CCM and related programs, such as RPM and PCM.


