



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Telemedicine software helps mid-market hospitals expand access through video-based visits, but it struggles to scale across departments, data, and care models.
- Virtual care platforms go further by connecting workflows, enabling continuous patient management, and aligning with value-based care.
- The real decision is not tool selection, but whether to keep adding visit-based solutions or build a digital care infrastructure that drives outcomes, efficiency, and long-term financial sustainability.
Is your telemedicine software actually scaling care or just adding more virtual visits?
That is the question many CIOs and digital health leaders are now facing. What started as a fast response to expand access has turned into a patchwork of tools, workflows, and disconnected data. Telemedicine software works well for visits, but as hospitals move toward value-based care and tighter margins, the limits become clear.
The real challenge is not adoption. It is knowing whether your current model can support continuous, coordinated care across populations.
I. What Is the Core Difference Between Telemedicine Software and Virtual Care Platforms?
The confusion is expensive.
Many mid-market hospitals believe they have scaled virtual care when they have only deployed telemedicine software across a few departments. It feels like progress. It looks like growth. But underneath, the architecture tells a different story.
What happens when a hospital scales telemedicine software across departments without aligning data, workflows, and compliance models?
Fragmentation creeps in. Costs rise quietly. Clinical continuity breaks.
The real risk is not adopting telemedicine software. It is scaling it without an architecture that supports longitudinal care.
This is where most CIOs pause.
Because the decision is no longer about adding another telehealth platform. It is about choosing between two fundamentally different models of care delivery.
A. How Is Telemedicine Software Defined in Today’s Healthcare Landscape?
At its core, telemedicine software is a visit tool.
It was built to solve one urgent problem: access.
During the pandemic, hospitals deployed telemedicine software rapidly to maintain care continuity. Video visits became the default entry point. For many organizations, that model still defines their digital strategy today.
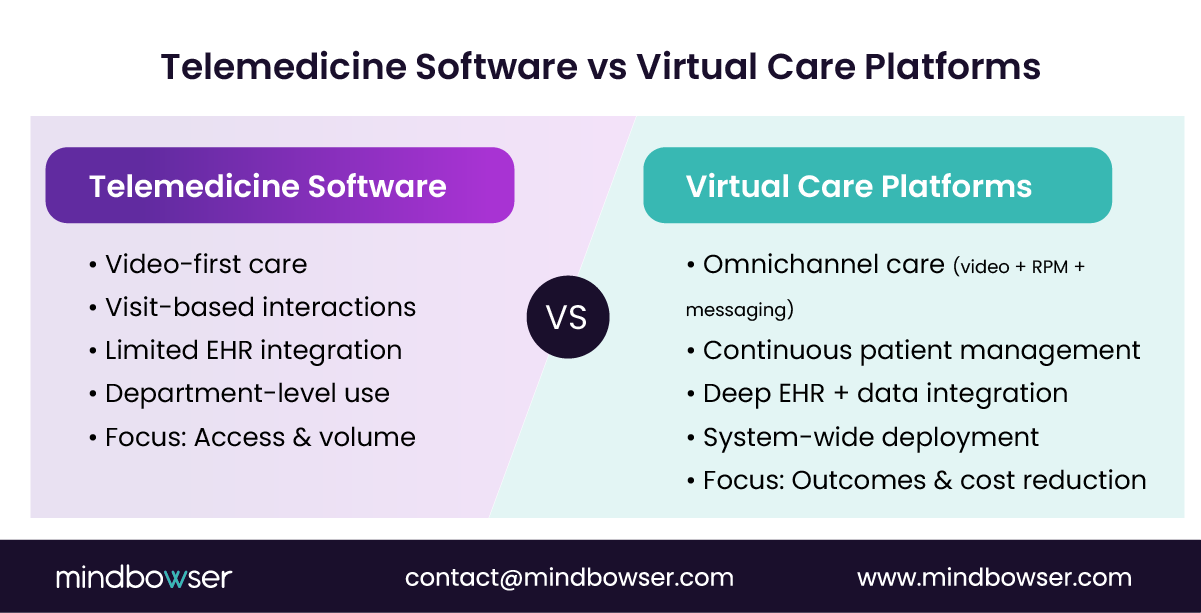
Here is what typically defines telemedicine software:
- Video-first care delivery
Real-time virtual visits powered by WebRTC or similar technologies. The interaction is clinician-to-patient and time-bound. - Basic clinical workflows
Scheduling and appointment management, ePrescriptions, and documentation with light EHR syncing. - Limited integration depth
Telemedicine software connects to EHRs, but often at a surface level. Data flows are transactional, not continuous. - Department-level deployment
Behavioral health, urgent care, and specialty clinics often run separate instances of telemedicine software. - Access expansion as the primary goal
Increase visit volume, reduce no-shows, and extend geographic reach.
Telemedicine software improves access. It does not manage care across time, risk, or populations.
Telemedicine software solves for visits, not outcomes.
B. What Defines a Full Virtual Care Platform?
A virtual care platform is infrastructure, not a feature.
It connects care across the entire patient journey: before the visit, during the visit, and after the visit.
That shift changes everything.
Instead of focusing on encounter volume, virtual care platforms focus on continuity, coordination, and outcomes.
Here is what defines them:
- Omnichannel care delivery
Video visits, remote patient monitoring (RPM), asynchronous messaging, and AI-driven triage and routing. - Continuous patient engagement
Patients are monitored and guided between visits. Data flows from devices, apps, and care teams into a unified system. - Care coordination layers
Providers, nurses, and care managers operate within shared workflows, reducing fragmentation. - Deep analytics and population health integration
Virtual care platforms connect directly to population health systems, enabling risk stratification and intervention tracking. - Unified digital care infrastructure
Instead of multiple tools, hospitals operate within a connected virtual care ecosystem.
Telemedicine software supports episodic care. Virtual care platforms support longitudinal care.
One expands access. The other drives outcomes.
And outcomes are what reimbursement is shifting toward.
Virtual care platforms align with value-based care. Telemedicine software alone does not.
C. Where Do Mid-Market Hospitals Typically Start?
Most hospitals did not plan their starting point. They reacted.
The rapid adoption of telemedicine software during COVID-19 created a patchwork of solutions across departments. Speed was prioritized. Architecture was deferred.
Now, that debt is visible.
Here is what we consistently see:
- Pandemic-driven deployment
Telemedicine software was rolled out quickly across high-demand specialties like behavioral health and primary care. - Fragmented pilots across departments
Different teams adopted different telehealth platforms, creating disconnected workflows. - Limited healthcare interoperability
Data remains siloed. Patient journeys are difficult to track across systems. - Visit-based ROI mindset
Success is measured by virtual visit volume, no-show reduction, and provider utilization. What is missing is cost-of-care reduction and long-term outcomes. - Emerging strategic pressure
Leadership is now asking a harder question: can our current telemedicine software scale into a true digital care infrastructure?
That is where friction begins.
Because scaling telemedicine software into a virtual care ecosystem is not a simple upgrade. It requires a shift in architecture, governance, and investment.
Mid-market hospitals start with telemedicine software. The challenge is knowing when it stops being enough.
II. How Do Architecture and Scalability Differ Between the Two Models?
This is where strategy becomes technical reality.
At first glance, telemedicine software and virtual care platforms may look similar. Both enable virtual visits. Both connect patients and providers. But under the hood, their architectures tell two completely different stories.
And architecture decides scale.
What happens when demand increases across specialties, locations, and care pathways?
One model stretches. The other breaks.
A. What Does the Technology Stack Look Like for Telemedicine Software?
Most telemedicine software is built for speed, not scale.
It prioritizes quick deployment and ease of use. That made sense in 2020. It becomes limiting in 2025.
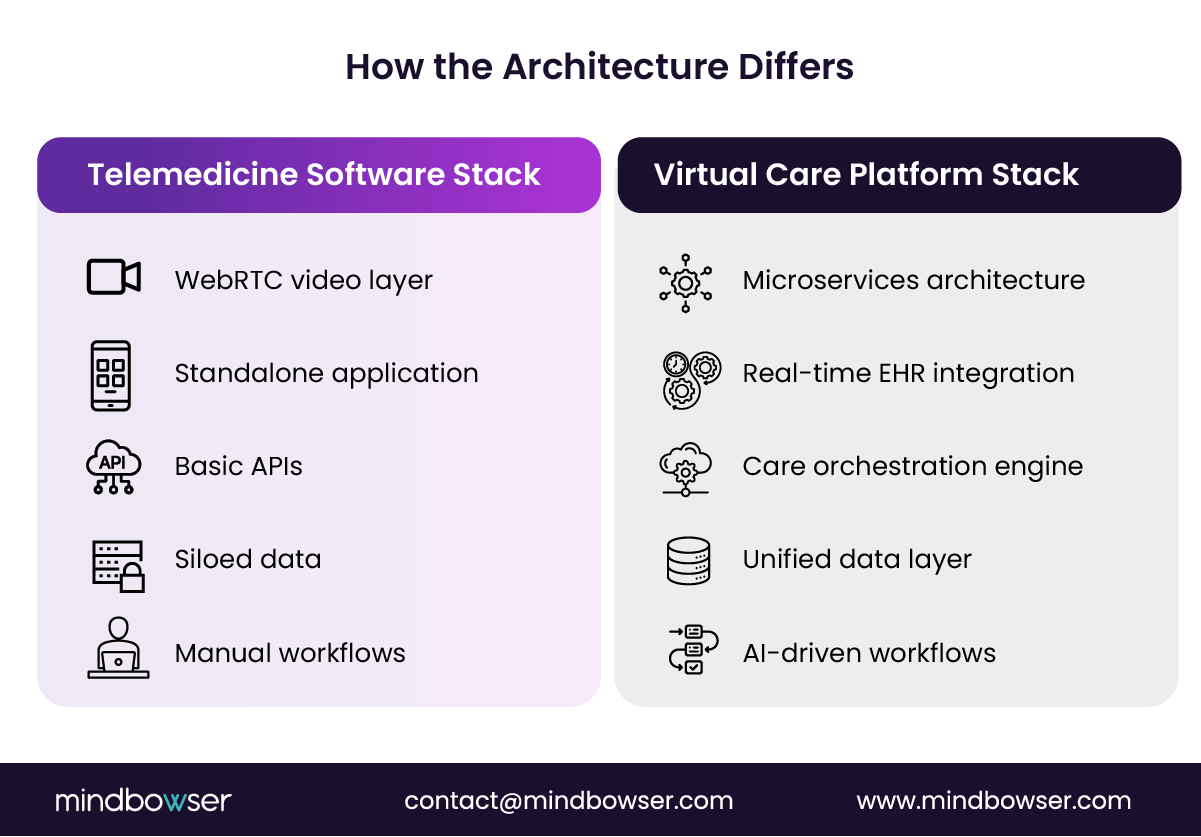
Here is what typically sits under the hood:
- WebRTC-based video infrastructure
Real-time communication engines power virtual visits. Reliable for 1:1 interactions, but not designed for complex orchestration. - Standalone application layers
Telemedicine software often runs as a separate system from core hospital infrastructure. It plugs in, but it does not integrate deeply. - Basic API integrations
EHR connectivity for scheduling or documentation, billing system hooks, and limited patient data exchange. These integrations are often one-way or batch-based. - Minimal workflow automation
Most workflows rely on manual coordination. Care teams step in to bridge gaps between systems. - Siloed data storage
Patient interaction data lives inside the telemedicine software environment, not across the full digital care infrastructure.
It works well for individual encounters. It struggles with continuity.
Telemedicine software is architected for isolated interactions, not system-wide orchestration.
B. How Is a Virtual Care Platform Architected for Enterprise Scale?
A virtual care platform is built like a health system, not a feature.
It treats virtual care as an extension of clinical operations, not a separate channel.
That changes the architecture completely.
Here is what defines a scalable virtual care platform:
- Microservices-based architecture
Each function runs independently, including scheduling, triage, RPM, messaging, and analytics. This allows hospitals to evolve components without breaking the system. - Deep EHR integration
Data flows bi-directionally and in real time. Patient records, care plans, and clinical notes stay synchronized across systems. - Care orchestration layers
Workflow engines coordinate patient routing, care team assignments, and escalation protocols. This replaces manual handoffs with structured pathways. - AI-driven workflows
Intelligent triage, risk scoring, and intervention triggers enable proactive care, not reactive visits. - Unified data layer for population health
All patient interactions feed into a centralized system that supports analytics, reporting, and quality metrics.
Telemedicine software connects people. Virtual care platforms connect systems, data, and decisions.
One is a tool. The other is infrastructure.
Virtual care platforms are designed for scale because they assume complexity from day one.
C. What Happens When Hospitals Attempt to Scale Basic Telemedicine Software?
This is where most mid-market hospitals feel the strain.
They try to extend telemedicine software beyond its original purpose. Add more departments. Add more use cases. Add more integrations.
And slowly, friction builds.
Here is what typically happens:
- Integration debt accumulates
Each new connection adds complexity. APIs become harder to maintain. Data mappings break. IT teams spend more time fixing than building. - Fragmented patient data
Clinical data lives across multiple systems. No single source of truth. Care teams lack full visibility into patient journeys. - Compliance risks increase
As systems multiply, so do risk points. HIPAA compliance becomes harder to enforce across disconnected tools. - Operational inefficiencies grow
Staff manually bridge gaps between systems. This increases workload, delays care, and introduces errors. - Vendor lock-in limits flexibility
Hospitals become dependent on telemedicine software vendors that were never designed to support enterprise-scale needs.
Here is the uncomfortable truth.
Scaling telemedicine software often creates more problems than it solves.
Because the cost is not just technical. It is clinical, financial, and strategic.
Pushing telemedicine software beyond its design leads to fragmentation, risk, and rising costs.
Want to Build a Scalable Virtual Care Platform for Your Hospital?
III. Which Model Aligns Better With Value-Based Care and Financial Sustainability?
Follow the money. It reveals the model.
Mid-market hospitals are under pressure from both sides. Fee-for-service revenue is tightening. Value-based care contracts are expanding. Margins are thin. Expectations are rising.
So the real question is not technical.
It is financial.
Which model helps you sustain revenue while reducing the cost of care?
A. How Does Telemedicine Software Impact Revenue and Cost?
Telemedicine software drives volume. That is its strength.
It expands access quickly. More appointments. More encounters. More billable events.
For hospitals operating primarily in fee-for-service environments, this matters.
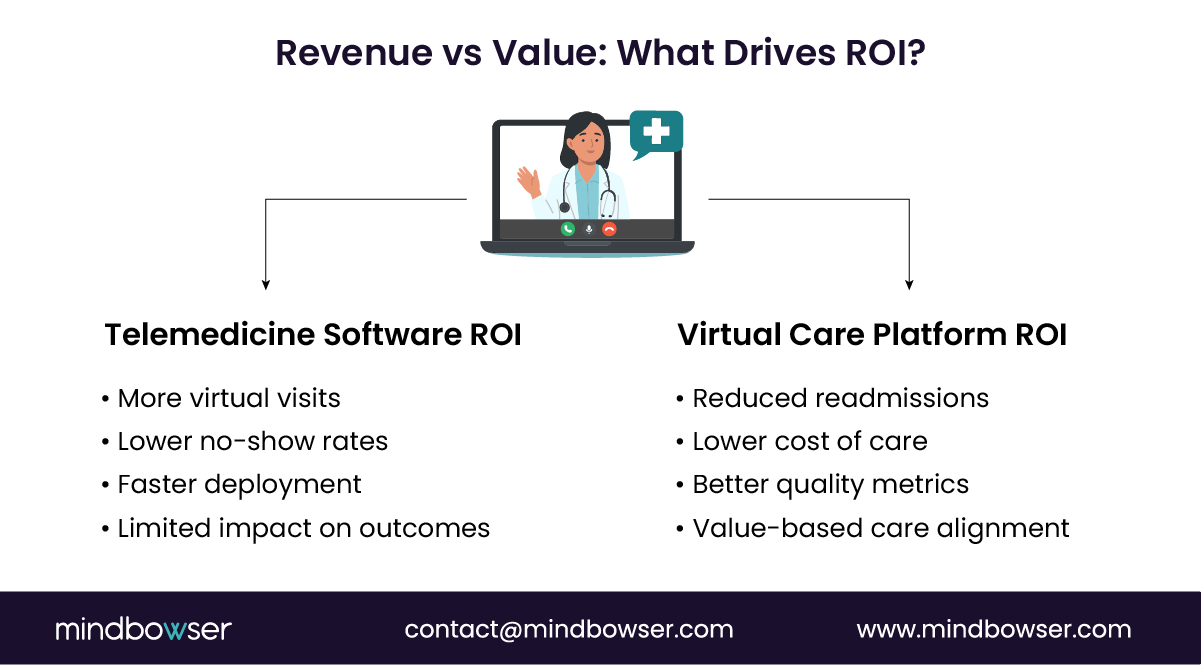
Here is how telemedicine software typically impacts financial performance:
- Visit-based revenue expansion
Telemedicine software increases appointment availability, allowing providers to see more patients without physical constraints. - Reduced no-show rates
Virtual visits improve patient convenience, leading to better attendance and more predictable scheduling. - Lower overhead per visit
Fewer physical resources are needed. Exam rooms, front desk coordination, and facility costs decrease. - Faster time to deploy and monetize
Hospitals can launch telemedicine software quickly and begin generating revenue within weeks.
But here is the constraint.
Telemedicine software revenue is tied to encounters. No visit, no revenue.
And in a value-based world, that model starts to weaken.
There is a limited impact on readmission reduction, chronic disease management, and total cost of care.
Telemedicine software supports fee-for-service growth but has limited influence on long-term cost and outcomes.
B. How Do Virtual Care Platforms Drive System-Level ROI?
Virtual care platforms shift the equation from volume to value.
They do not depend solely on visits. They generate ROI across the entire care continuum.
This is where mid-market hospitals begin to see strategic leverage.
Here is how virtual care platforms drive financial impact:
- Remote patient monitoring (RPM) reduces readmissions
Continuous monitoring allows early intervention. Chronic conditions are managed before they escalate. - Care coordination lowers utilization costs
Patients are guided to the right level of care. Avoidable ER visits and unnecessary admissions decrease. - Improved quality metrics and reimbursement alignment
Virtual care platforms support HEDIS measures, CMS quality programs, and shared savings models. - Population health management at scale
Hospitals can stratify risk, target interventions, and manage cohorts instead of individual visits. - Operational efficiency across care teams
Automated workflows reduce manual effort, freeing clinical staff to focus on higher-value tasks.
Telemedicine software generates episodic revenue. Virtual care platforms generate system-level savings and performance gains.
One feeds volume. The other improves the margin.
And margin is where survival lives.
Virtual care platforms align directly with value-based care economics and long-term sustainability.
C. What Do Industry Signals Suggest About the Future?
The direction is clear, even if the transition is messy.
Healthcare is moving away from isolated encounters and toward continuous care models. Policy, payers, and providers are all pushing in the same direction.
Here are the signals CIOs and digital leaders should not ignore:
- CMS reimbursement evolution
Expanded support for RPM, chronic care management, and virtual services beyond traditional visits. - Payer pressure on outcomes and cost control
Contracts increasingly tie reimbursement to performance metrics, not just service delivery. - Consolidation of the virtual care ecosystem
Hospitals are moving away from fragmented telehealth platforms toward unified systems. - Shift in CIO strategy from tools to infrastructure
Leadership is prioritizing digital care infrastructure that supports longitudinal patient management. - Rising demand for healthcare interoperability
Data must move seamlessly across systems to support coordinated care and reporting.
Here is the uncomfortable insight.
Hospitals that rely only on telemedicine software risk falling behind as reimbursement models evolve.
Because access alone is no longer enough.
Outcomes decide revenue. The future favors integrated virtual care platforms, not isolated telemedicine software.
IV. What Decision Framework Should Mid-Market Hospitals Use?
This is where good intentions meet hard trade-offs.
Every CIO and CMIO eventually reaches the same point.
The current telemedicine software works. Clinicians use it. Patients accept it. Revenue flows.
So why change?
Because the question is no longer whether it works. It is whether it will scale across care models, contracts, and populations.
That shift requires a decision framework, not a vendor demo.
A. What Strategic Questions Should CIOs and CMIOs Ask?
The right questions prevent expensive rewrites later.
Before expanding telemedicine software or investing in virtual care platforms, leadership teams should align on a few critical decisions.
Ask these:
- Are we optimizing for visit volume or patient outcomes?
This defines whether telemedicine software is enough or if a broader virtual care ecosystem is required. - Can our current telemedicine software support longitudinal care pathways?
Think chronic care, post-discharge monitoring, and multi-touch engagement. - How deep is our healthcare interoperability today?
Consider real-time EHR sync, device data integration, and cross-department visibility. - What is our exposure to value-based contracts over the next 3 to 5 years?
The higher the exposure, the greater the need for coordinated virtual care platforms. - Where is our operational friction today?
Look for manual workflows, data silos, and care coordination gaps. - Do we control our digital care infrastructure or depend on vendor limitations?
This question alone often reshapes the entire strategy. - What is the cost of doing nothing for the next 24 months?
Not upgrading telemedicine software has a cost. It shows up in missed savings, inefficiencies, and lost contracts.
Most hospitals realize they are not choosing between tools. They are choosing between operating models.
The right questions expose whether telemedicine software is a bridge or a bottleneck.
B. How Should Hospitals Evaluate Build vs. Platform vs. Custom Hybrid?
There is no single right answer. Only aligned answers.
Hospitals typically evaluate three paths when moving beyond basic telemedicine software:
- Off-the-shelf telehealth platforms
- Full virtual care platforms
- Custom-built or hybrid digital care infrastructure
Each comes with trade-offs.
Off-the-shelf telemedicine software is fast to deploy, lower in upfront cost, and familiar to use. But it often brings limited customization, shallow integrations, and difficulty scaling across complex care models.
Pre-built virtual care platforms offer broader capabilities out of the box. But they can come with expensive licensing models, rigid workflows, and only partial alignment with hospital-specific needs.
The custom hybrid approach is increasingly preferred. It combines telemedicine software components with custom-built orchestration, integrations, and workflows. This allows hospitals to control their digital care infrastructure, align with specialty workflows, and integrate deeply with existing systems.
| Model | Speed to Deploy | Flexibility | Scalability | Cost Over Time | Control |
|---|---|---|---|---|---|
| Telemedicine Software | High | Low | Limited | Medium | Low |
| Virtual Care Platform (Pre-built) | Medium | Medium | High | High | Medium |
| Custom Hybrid Model | Medium | High | Very High | Optimized | High |
Here is the insight most teams miss.
Speed feels good early. Control matters later.
Mid-market hospitals often win with a custom hybrid approach that extends telemedicine software into a scalable virtual care ecosystem.
V. How Mindbowser Helps Mid-Market Hospitals Move Beyond Basic Telemedicine
Most hospitals do not fail at vision. They fail at execution.
Leadership teams understand the gap. They see the limits of telemedicine software. They know virtual care platforms are the direction.
But the transition is where things break.
Too many vendors push rigid platforms. Too many internal teams underestimate the complexity of integration. And too many projects stall between pilot and scale.
That is where a custom-built approach changes the outcome.
A. Designing Scalable Telemedicine Foundations
Start with what works. Then rebuild what does not scale.
Mindbowser does not blindly replace telemedicine software. It strengthens the foundation so it can evolve into a true digital care infrastructure.
Here is how:
- Custom architecture aligned to hospital workflows
Instead of forcing clinicians into generic tools, telemedicine software is extended to match specialty-specific workflows. Cardiology is not behavioral health. The system should reflect that. - HIPAA and SOC 2 compliance by design
Security is built into the architecture, not added later. This reduces risk as virtual care expands across departments and use cases. - Deep integration with existing systems
Real-time EHR synchronization, billing, and revenue cycle alignment, and device plus RPM data ingestion. This removes silos created by standalone telemedicine software deployments. - Modular scalability
Hospitals can expand capabilities without replacing core systems. Add RPM. Add care coordination. Add analytics. No full rebuild required.
Telemedicine software stops being a tool. It becomes part of a larger system.
A strong foundation allows telemedicine software to scale without creating technical debt.
B. Transforming Telemedicine into a Full Virtual Care Ecosystem
This is where real value emerges.
Once the foundation is in place, telemedicine software evolves into a connected virtual care ecosystem. Not overnight, but intentionally.
Here is how Mindbowser drives that transformation:
- Remote patient monitoring (RPM) integration
Continuous data from devices feeds directly into care workflows. Clinicians move from reactive visits to proactive management. - AI-driven triage and care pathways
Intelligent routing ensures patients receive the right care at the right time. This reduces unnecessary utilization and improves outcomes. - Care coordination across teams
Nurses, care managers, and specialists operate within unified workflows instead of disconnected systems. - HealthConnect CoPilot acceleration layer
Pre-built accelerators reduce build time by up to 40%, allowing hospitals to scale faster without sacrificing customization. - Population health alignment
Data flows into analytics systems that support risk stratification, quality metrics, and value-based care performance.
This is not about adding features to telemedicine software.
It is about connecting care across time, teams, and touchpoints.
Telemedicine software becomes a gateway, not the destination.
C. Real-World Implementation Patterns
The model works because it adapts to real hospital constraints.
Mid-market hospitals do not transform everything at once. They scale in focused, high-impact areas.
Here are common patterns we see:
- Behavioral health scaling
Telemedicine software starts with video visits, then expands into longitudinal care with therapy tracking, asynchronous check-ins, and care coordination. - Chronic care with RPM
Patients with diabetes, hypertension, or heart conditions are monitored continuously. Interventions happen before acute events. - Multi-location system consolidation
Hospitals unify multiple telehealth platforms into a single digital care infrastructure, reducing fragmentation and operational overhead. - Post-discharge care pathways
Virtual follow-ups, monitoring, and care coordination reduce readmissions and improve patient outcomes. - Specialty-driven virtual clinics
High-margin specialties extend care beyond physical locations using integrated virtual care models.
Real-world success comes from phased evolution, not disruptive replacement.
What Will Actually Scale in 2025 and Beyond?
Telemedicine software opened the door to access, but access alone will not sustain margins or meet value-based expectations. Mid-market hospitals that continue layering telemedicine software without rethinking architecture will face rising costs, fragmented data, and limited impact on outcomes.
The shift now is from tools to infrastructure, from visits to continuity, and from volume to accountability.
Virtual care platforms, or custom-built ecosystems around telemedicine software, are what enable that shift. The decision is simple, even if the path is not: keep extending a visit tool, or build a system that manages care across time.
Telemedicine software vendors focus on video visits and basic workflows for quick deployment. Virtual care platform providers offer broader systems that support care coordination, analytics, and continuous patient management.
Hospitals need cross-functional alignment across IT, clinical leadership, operations, and compliance. Scaling fails when virtual care is treated as only an IT initiative.
Telemedicine software delivers a visit-based experience with limited follow-up. Virtual care platforms create continuous engagement through monitoring, reminders, and coordinated care journeys.
Hidden costs include integration maintenance, manual workflows, and fragmented data management. Over time, these reduce efficiency and increase operational overhead.
The shift should happen when systems become fragmented and care coordination breaks down. Rising value-based care exposure and inefficiencies are strong signals to move beyond telemedicine software.


