



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 
























TL;DR
HEDIS (Healthcare Effectiveness Data and Information Set) measures set the standard for healthcare quality in the United States, defining how plans and providers measure, report, and improve care. Given the scale of HEDIS, used by 90% of U.S. health plans and impacting 200 million covered lives, even incremental changes carry national consequences.
As the industry moves into HEDIS Measurement Year (MY) 2026, organizations face a pivotal shift. Reporting expectations are tightening, equity requirements are more explicit, and digital submission is no longer optional.
Understanding what changed, why it matters, and how to prepare is essential for maintaining compliance, protecting revenue, and staying aligned with NCQA and CMS expectations.
HEDIS measures are updated annually by the National Committee for Quality Assurance (NCQA) to reflect evolving clinical evidence, regulatory priorities, and data capabilities. These updates influence payer contracts, provider workflows, quality bonuses, and accreditation outcomes.
This guide breaks down what changed from MY 2025 to MY 2026, explains key acronyms and measures, and outlines a practical readiness path for payers and providers navigating the 2026 reporting year.

I. HEDIS MY 2025 in Review
HEDIS MY 2025 functioned as a transitional year, bridging legacy reporting approaches with the stricter digital and equity-driven requirements that follow in MY 2026.
While organizations retained some operational flexibility in 2025, NCQA used this measurement year to signal a clear direction on reporting rigor, data completeness, and accountability.
A. What Defined MY 2025
Several themes shaped MY 2025 performance and preparation:
- Gradual retirement of legacy measures, with clear notice of upcoming replacements
- Expanded reliance on Electronic Clinical Data Systems (ECDS), though hybrid reporting remained in limited use
- Initial refinement of health equity stratification, setting expectations for cleaner demographic data
MY 2025 exposed where quality programs were resilient and where manual or fragmented processes could no longer keep pace.
B. Key Measure Changes Observed in MY 2025
MY 2025 introduced or advanced changes that directly influenced clinical workflows and reporting strategies:
- Early transition from CBP to BPC-E, signaling a more precise approach to blood pressure control
- Introduction of DBM-E and FMA-E, expanding focus on women’s health through digital mammography and follow-up tracking
- Expanded behavioral health emphasis, with measures such as IET and FUM receiving greater operational and reporting attention
These updates required tighter alignment between care delivery, documentation, and quality reporting teams.
1. Operational Lessons from MY 2025
Performance outcomes from MY 2025 highlighted consistent patterns across payers and providers:
- Organizations that reviewed specifications early identified fewer downstream data gaps
- Teams that tested ECDS workflows ahead of submission reduced audit risk and rework
- Incomplete race and ethnicity data emerged as a recurring weakness across reporting entities
At the same time, MY 2025 revealed persistent challenges, including misaligned workflows, delayed data ingestion, and continued reliance on manual validation steps.
2. Why MY 2025 Still Matters
MY 2025 serves as the baseline for MY 2026 readiness. The gaps identified, measures transitioned, and workflows tested during 2025 directly inform an organization’s ability to comply with expanded ECDS-only reporting and refined equity requirements.
In practical terms, MY 2025 represented the final adjustment period. MY 2026 formalizes the expectations introduced during this review year.
II. HEDIS 2025 vs 2026 — Comparative Breakdown
The table below summarizes how HEDIS evolved from MY 2025 into MY 2026, highlighting changes that directly affect reporting operations, accreditation outcomes, and quality strategy.
MY 2026 reflects tighter enforcement of standards that were introduced or previewed in prior years.
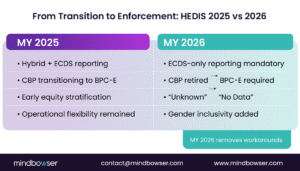
These changes confirm that MY 2026 is not an incremental update. It represents a firm shift toward standardized digital reporting, clearer equity definitions, and stronger linkage between HEDIS performance, accreditation status, and Star Ratings outcomes.
III. Key HEDIS Measures and Acronyms Explained (MY 2026)
HEDIS reporting relies on a dense set of acronyms that carry specific clinical and technical meaning.
For MY 2026, understanding which measures remain active, which have transitioned, and which are now mandatory under ECDS-only reporting is essential for accurate submission and audit readiness.
A. Cardiovascular and Chronic Disease Measures
These measures continue to anchor HEDIS performance, particularly as CBP fully transitions to BPC-E in MY 2026.
- CBP – Controlling High Blood Pressure
Retired in MY 2026. CBP is no longer reportable and has been formally replaced by BPC-E. - BPC-E – Blood Pressure Control for Adults
The required hypertension measure in MY 2026. BPC-E replaces CBP and emphasizes consistent, electronically captured blood pressure data suitable for ECDS-only reporting. - SPC – Statin Therapy for Patients With Cardiovascular Disease
Measures appropriate statin use in patients with established cardiovascular disease. SPC remains active and unchanged in MY 2026. - OMW – Osteoporosis Management in Women Who Had a Fracture
Focuses on post-fracture osteoporosis care in older women. OMW remains active with streamlined specifications. - PCR – Persistence of Beta-Blocker Treatment After a Heart Attack
Evaluates the continuity of beta-blocker therapy following myocardial infarction. PCR remains an active cardiovascular quality measure.
B. Women’s Health and Preventive Care Measures
MY 2026 expands emphasis on women’s health through digital-first screening and follow-up measures.
- DBM-E – Digital Breast Mammogram
Measures the use of digital mammography for breast cancer screening. DBM-E is active and aligned with ECDS-only workflows. - FMA-E – Follow-Up After Mammogram
Tracks timely follow-up after abnormal mammogram results. This measure requires a reliable linkage between imaging orders and follow-up care. - PPC – Prenatal and Postpartum Care
Assesses timely prenatal and postpartum visits. PPC remains active in MY 2026. - COA – Care for Older Adults
Evaluates multiple domains of care for older adults, including functional status and medication review. - WCC – Weight Assessment and Counseling for Children and Adolescents
Measures BMI assessment and counseling in pediatric populations.
C. Behavioral Health and Substance Use Measures
Behavioral health measures continue to expand in importance and operational visibility in MY 2026.
- IET – Initiation and Engagement of Alcohol and Other Drug Treatment
Measures timely initiation and ongoing engagement in substance use treatment. - FUM – Follow-Up After Emergency Department Visit for Mental Illness
Evaluates whether patients receive follow-up care after an ED visit for mental health conditions. - HBD – Depression Screening and Follow-Up for Adolescents and Adults
Measures depression screening and appropriate follow-up actions.
D. Digital and Equity-Driven Measures

MY 2026 reinforces digital submission and equity stratification expectations across applicable measures.
- ECDS – Electronic Clinical Data Systems
The required reporting method for most HEDIS measures in MY 2026. ECDS-only reporting eliminates reliance on manual chart abstraction. - EED – Depression Screening Using ECDS
A digital-first depression screening measure that depends on structured electronic data sources. - APM – Adult Preventive Measures
A composite measure covering preventive services and screenings for adult populations. - KED – Kidney Health Evaluation for Patients With Diabetes
Assesses kidney disease screening and monitoring in patients with diabetes.
E. Key Transition to Note
- CBP → BPC-E: CBP is fully retired in MY 2026. All hypertension reporting must use BPC-E.
- ECDS-only reporting is mandatory for most measures, requiring structured, interoperable data across clinical systems.
- Women’s health and behavioral health measures are expected to carry increased reporting and data integration requirements in MY 2026.
IV. Technical Requirements and Preparation Roadmap for HEDIS MY 2026
HEDIS MY 2026 introduces technical requirements that leave little room for manual intervention.
Reporting success now depends on the availability of structured data, the maturity of interoperability, and disciplined preparation timelines. Organizations that approach MY 2026 as a technical compliance exercise rather than a quality project face elevated risk.

ECDS Reporting Requirements in MY 2026
For MY 2026, ECDS-only reporting is mandatory for most HEDIS measures. Hybrid models that relied on chart abstraction are no longer sufficient at scale.
What ECDS-only means operationally:
- Data must be electronically captured, structured, and retrievable
- Source systems typically include EHRs, registries, health information exchanges, and claims systems
- Manual chart review cannot be used to “fill gaps” for most measures
This requirement raises the bar for data governance, mapping accuracy, and system integration.
V. Core Technical Expectations
Organizations preparing for MY 2026 should validate readiness across the following areas:
- Structured clinical documentation for blood pressure, mammography results, behavioral health encounters, and follow-up care
- Interoperability standards supporting ECDS workflows, including HL7, C-CDA, and FHIR-based exchanges
- Consistent coding and mapping to support measure logic without manual remediation
- Audit-ready data lineage, ensuring reported values can be traced back to source systems
Measures such as BPC-E, DBM-E, and FMA-E are particularly sensitive to documentation gaps and system handoffs.
VI. Preparation Timeline for MY 2026
HEDIS readiness for MY 2026 follows a predictable cadence. Organizations that align early reduce compliance pressure later.
Preparation Timeline
- Summer 2025: NCQA releases MY 2026 specifications
- Fall 2025: Workflow audits, data gap analysis, and ECDS validation
- January 1, 2026: MY 2026 measurement year begins
- Summer 2026: HEDIS MY 2026 submissions due
This timeline reinforces the need to complete technical remediation before the measurement year begins.
VII. Recommended Preparation Roadmap

1. Review MY 2026 Specifications Early
Identify new requirements, measure logic changes, and retire measures. Pay close attention to ECDS eligibility rules.
2. Conduct Targeted Data Gap Analysis
Focus on high-risk measures:
- Blood pressure capture for BPC-E
- Mammography order-to-result and follow-up loops for DBM-E and FMA-E
- Behavioral health follow-up documentation for IET and FUM
3. Validate ECDS Infrastructure
Confirm that EHRs, registries, and downstream reporting tools can exchange and normalize structured data without manual intervention.
4. Align Clinical and Quality Workflows
Ensure frontline documentation supports measure logic. Misalignment at the point of care cannot be corrected downstream in MY 2026.
5. Test Early and Often
Run pilot extracts and mock submissions well before the submission window to surface data integrity issues.
6. Why Preparation Matters More in MY 2026
MY 2026 tightens the connection between technical readiness and organizational outcomes. HEDIS performance is directly tied to NCQA accreditation and CMS Star Ratings, increasing financial and regulatory exposure for incomplete or inaccurate submissions.
In effect, MY 2026 turns reporting maturity into a core compliance requirement, not a quality improvement option.
Empower Preventive Care with Smarter Workflows
Leverage AI-driven automation to track BPC-E, FMA-E, and behavioral health measures effortlessly—so your clinicians can focus on what matters most: patient outcomes.
HEDIS MY 2026 Readiness
HEDIS MY 2026 formalizes changes that have been in the works for several years. The transition to ECDS-only reporting, the full replacement of CBP with BPC-E, expanded women’s health measures, and tighter equity data standards collectively raise the compliance bar.
These updates apply at the national scale, given that HEDIS is used by 90% of U.S. health plans and impacts 200 million covered lives.
MY 2026 also reinforces the downstream impact of HEDIS performance. Results are directly tied to NCQA accreditation and CMS Star Ratings, increasing financial, regulatory, and reputational exposure for incomplete or inaccurate reporting. Organizations that rely on manual remediation, fragmented data pipelines, or incomplete demographic capture face heightened risk.
In practical terms, MY 2026 shifts HEDIS from a quality reporting exercise to a core operational compliance requirement. Success depends on structured documentation, interoperable systems, and early preparation aligned to NCQA timelines.
Yes. For MY 2026, ECDS-only reporting is mandatory for most HEDIS measures, significantly limiting the use of hybrid or manual chart abstraction.
CBP is retired and fully replaced by BPC-E (Blood Pressure Control for Adults) in MY 2026. Hypertension reporting must now follow BPC-E specifications.
MY 2026 includes DBM-E (Digital Breast Mammogram) and FMA-E (Follow-Up After Mammogram), expanding requirements for digital imaging and documented follow-up care.
The race and ethnicity category “Unknown” is replaced with “No Data”, increasing transparency around missing demographic information and strengthening equity analysis requirements.
Yes. Gender inclusivity has been added to applicable measures, requiring systems and reporting logic to reflect gender identity accurately.
Preparation should begin when MY 2026 specifications are released in Summer 2025, with technical validation completed before the measurement year starts on January 1, 2026, and submissions due in Summer 2026.


