



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Telemedicine urgent care platforms are redefining same-day virtual visits.
- For growth-stage digital health startups, custom development is the difference between scaling cleanly and stalling under vendor limits.
- Purpose-built platforms give you compliance by design, real EHR interoperability, predictable unit economics, and the freedom to evolve beyond basic video visits as the market accelerates
“The real question is not whether telemedicine urgent care works”
That debate is over.
The question Series B CTOs and co-founders are now asking is far more practical:
Do we build this as a core platform we own, or keep patching together tools that were never designed to scale with us?
As urgent care shifts from pandemic response to permanent care front door, the technical and economic stakes change. What once passed for “good enough” video and scheduling now becomes a constraint on compliance, integration, and growth.
Before deciding how to build, it’s critical to understand what telemedicine urgent care is and what it requires of the underlying platform.
What Is Telemedicine Urgent Care?
Telemedicine urgent care refers to real-time virtual clinical encounters designed for low acuity, high-frequency medical needs. These are not scheduled primary care visits and not emergency interventions. They sit squarely in the middle—fast, episodic, and outcome-driven.
At its core, telemedicine urgent care replaces the traditional walk-in clinic with a digital front door that operates on demand.
Clear definition
Telemedicine urgent care delivers:
- Live audio-video consultations with licensed clinicians
- Same-day access, often within minutes
- Protocol-driven care for conditions that do not require physical exams or imaging
From a technical standpoint, this means synchronous video, real-time documentation, ePrescribing, and billing workflows that must operate without delays or handoffs.
Common Clinical Use Cases
These platforms focus on repeatable, high-volume conditions, including:
- Upper respiratory infections, flu, and COVID follow-ups
- UTIs, rashes, skin infections
- GI issues, allergies, and minor injuries
- Post-discharge check-ins
- Chronic condition touchpoints, like asthma or diabetes coaching
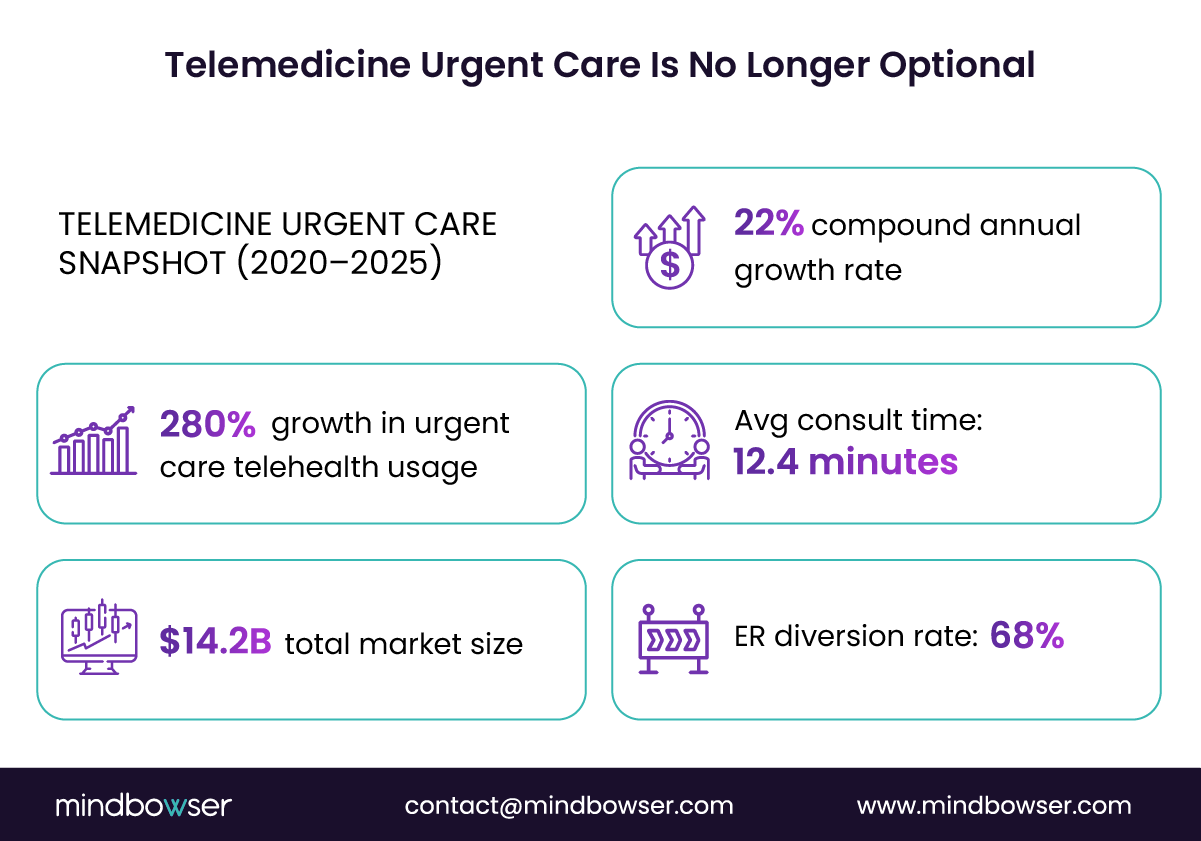
These use cases explain why the category exploded. Between 2020 and 2025, urgent care telehealth utilization grew by 280 percent, expanding into a $14.2B market with a 22 percent compound annual growth rate, according to McKinsey and JAMA healthcare market analyses published in 2025.
Why Urgent Care Works So Well Virtually
Urgent care is uniquely suited for telemedicine because:
- Decision trees are predictable
Most visits follow well-defined clinical pathways, making them ideal for digital triage and standardization. - Speed matters more than continuity
Patients want relief and reassurance now, not longitudinal care planning. - Clinical outcomes remain strong
Studies consistently show comparable outcomes for low-acuity conditions managed virtually.
Quantifiable System-level Value
From a health system and payer perspective, the value is measurable:
- 68 percent reduction in avoidable ER visits when urgent care telemedicine is used as a front door
- Average consult duration of 12.4 minutes, compared to 45 minutes or more for in-person urgent care
- Higher clinician utilization with fewer idle gaps
For startups, this creates a powerful flywheel. High frequency usage drives data, data drives product intelligence, and intelligence drives defensibility.
Telemedicine urgent care is not just video visits. It is a high-throughput care delivery system. When built correctly, it becomes one of the most capital-efficient growth engines in digital health.
Why Startups Are Investing in Custom Platforms
By the time a digital health startup reaches Series B, the problem is rarely demand. The problem is constraint. CTOs and co-founders are realizing that the telemedicine urgent care stack they launched is quietly dictating what the business can and cannot become.
Off-the-shelf tools create speed early. They also create ceilings.
The Hidden Cost of Third-party Dependency
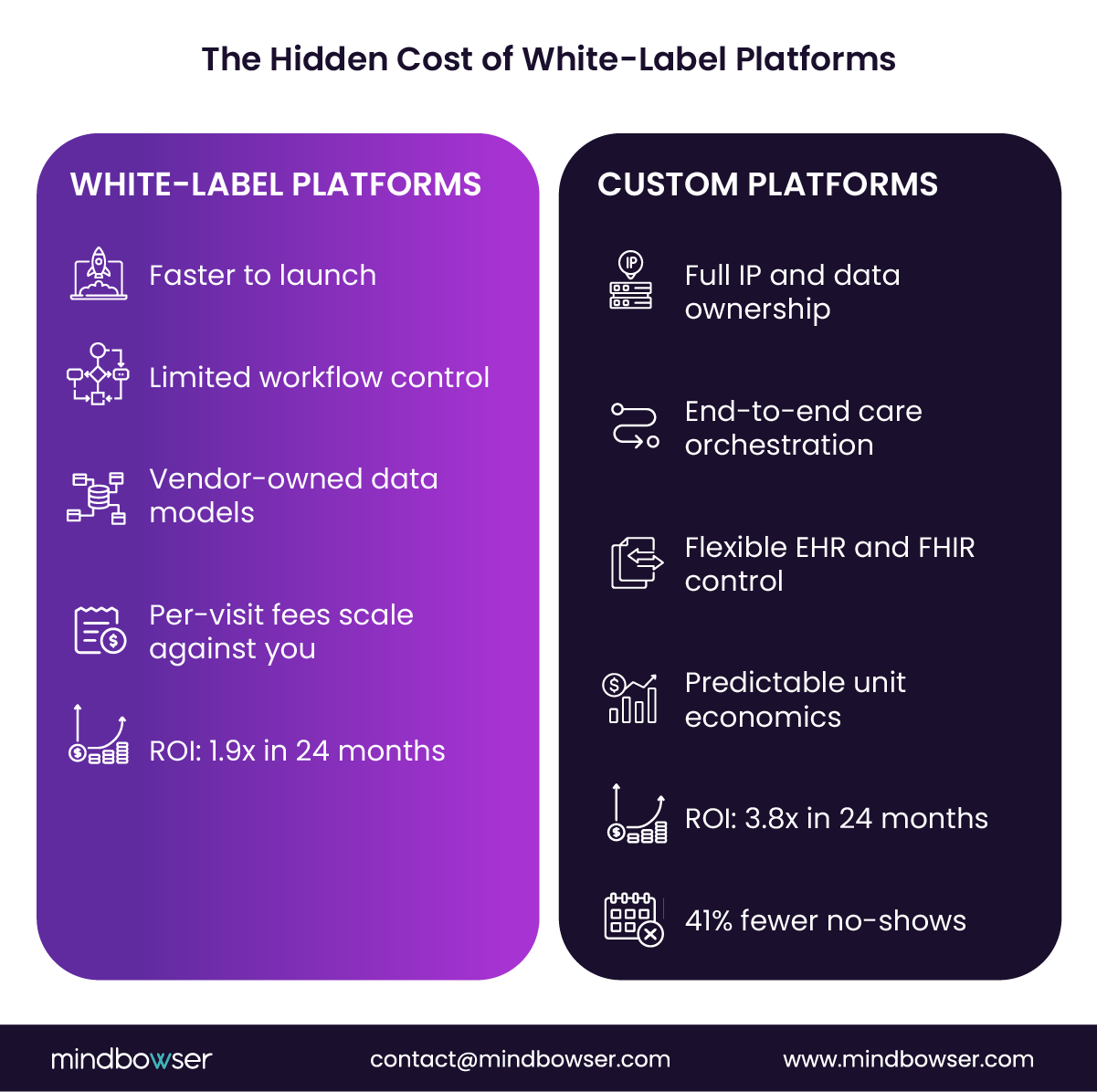
White-label telehealth platforms abstract away complexity, but they also abstract away control. Over time, that shows up in four painful ways:
- Data lock-in where clinical, operational, and behavioral data live in vendor schemas
- Roadmap misalignment, where your growth priorities compete with those of hundreds of other customers
- Limited extensibility when you want to add AI triage, new care models, or payer logic
- Margin compression from per-visit or per-provider fees that scale against you
For urgent care, which thrives on volume and repeat usage, these costs compound quickly.
Custom platforms flip the equation. You own the data, the workflows, and the economics. That ownership becomes strategic once investors start asking how defensible the product really is.
Building the Full Urgent Care Journey
Urgent care is not a single interaction. High-performing startups design it as a continuous flow:
- Digital intake and symptom triage
- Real-time clinician consult
- Documentation and clinical decision support
- ePrescribing and pharmacy routing
- Billing, eligibility, and claims
- Follow-ups, outcomes tracking, and retention loops
Off-the-shelf tools handle pieces of this. Custom platforms orchestrate everything in a single system. That orchestration is what reduces latency, no-shows, and drop-offs.
A 2024 analysis in the New England Journal of Medicine found that custom telemedicine platforms generated a 3.8x ROI within 24 months, compared to 1.9x for white-label solutions, largely due to tighter workflow control and a 41 percent reduction in no-show rates.
EHR and FHIR Are Not Plug-and-play
Most vendors advertise “FHIR compatible” integrations. In practice, they expose a narrow slice of what urgent care teams actually need.
With FHIR R4 now covering 87 percent of common EHR integration requirements, startups want the freedom to decide:
- Which resources to persist internally
- How to normalize data across multiple EHR partners
- Where to embed clinical logic versus external systems
Custom platforms let engineering teams treat interoperability as a first-class system, not a vendor constraint.
Investor and Enterprise Pressure
There is also a non-technical driver: diligence. Buyers, payers, and investors increasingly view platform ownership as a risk signal if your core urgent care workflows run on third-party rails, valuation and exit options narrow.
Startups invest in custom telemedicine urgent care platforms because growth demands control. Control over data. Control over compliance. Control over how fast the product can evolve when the market shifts again.
Common Challenges in Development
Building a custom telemedicine urgent care platform is not hard because of code volume. It is hard because every decision sits at the intersection of regulation, real-time systems, and clinical risk. This is where many Series B teams feel the most engineering strain.
Compliance Is Architectural, Not a Checklist
Urgent care telemedicine operates under overlapping regulatory regimes. HIPAA is the baseline. It is only the beginning.
Teams must account for:
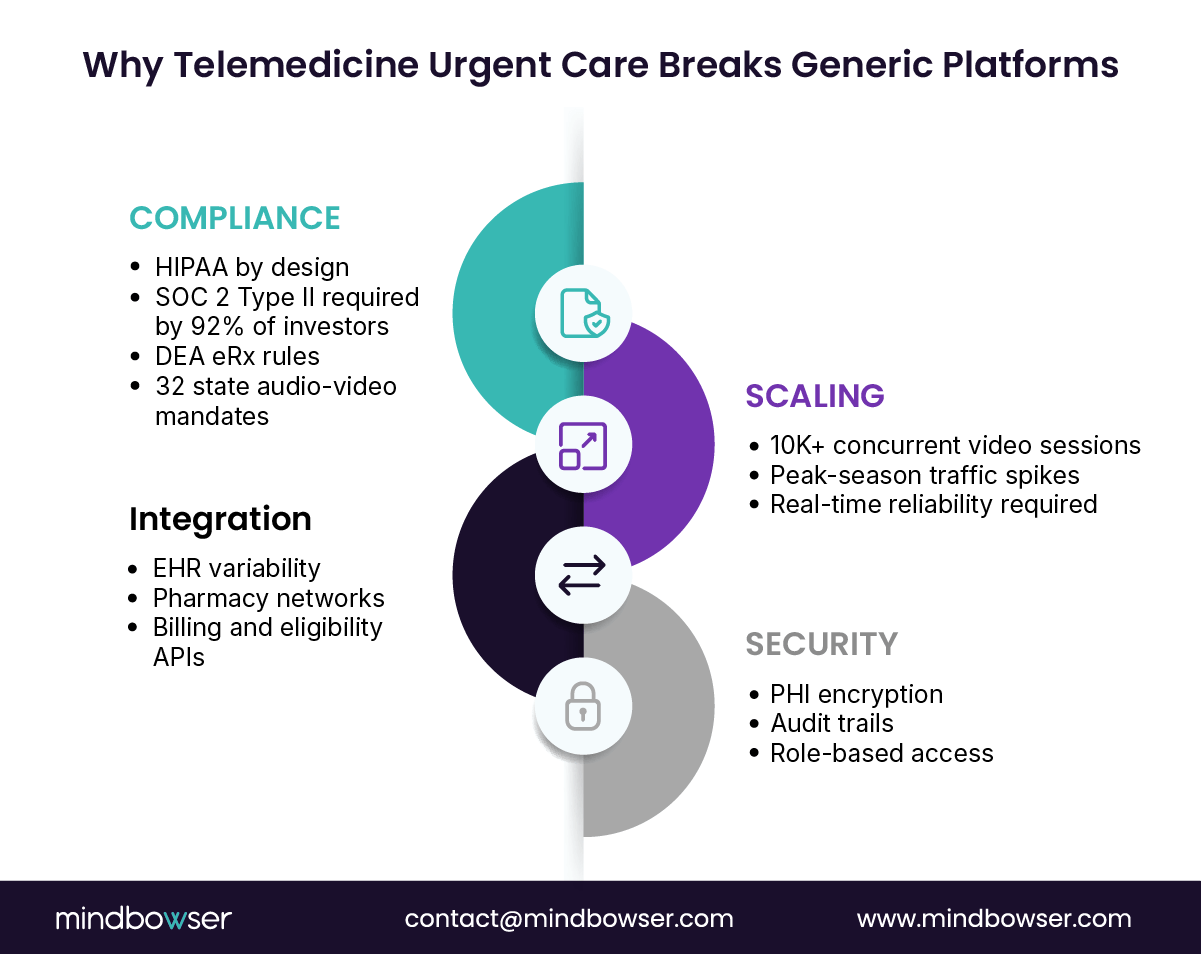
- HIPAA and HITECH requirements for PHI handling
- DEA rules for ePrescribing, especially controlled substances
- Audio-video visit mandates across 32 U.S. states, which affect how encounters are initiated and documented
- SOC 2 Type II controls are now included in 92% of investor and enterprise due diligence processes, according to HHS- and DEA-aligned reviews.
The mistake many teams make is treating compliance as a post-MVP hardening phase. In reality, compliance decisions shape identity management, logging, data retention, and even UI flows. Retrofitting later slows releases and raises audit risk.
Scaling Real-time Video Without Degradation
Urgent care traffic is inherently bursty. Seasonal illnesses, employer launches, and regional outbreaks can cause sudden load spikes.
Modern WebRTC infrastructure can technically support scale. Benchmarks from AWS show WebRTC architectures can handle 15,000 concurrent HD video sessions when properly configured. The challenge is everything around the video:
- Session orchestration
- Failover and reconnect logic
- Bandwidth management across devices
- Latency under geographic dispersion
Without deliberate load modeling and cloud architecture, quality drops right when demand peaks.
Integration Complexity Compounds Quickly
Urgent care platforms sit in the middle of a dense integration web:
- EHR systems for documentation and continuity
- Pharmacy networks for eRx
- Eligibility and billing systems
- Payment gateways for consumer pay models
While FHIR R4 now supports 87 percent of common EHR integration needs, real-world implementations vary widely. Each partner interprets resources slightly differently. Without a normalization layer, engineering teams end up writing brittle, one-off logic that slows every future integration.
Security and Audit Readiness
Beyond encryption, mature urgent care platforms require:
- End-to-end audit trails for every clinical action
- Role-based access tied to licensure and scope of practice
- Breach detection and response logging aligned with SOC 2 controls
These features rarely show up in early demos, but they surface immediately during enterprise sales and investor diligence.
The biggest challenge in the development of telemedicine urgent care is not speed. It is building a system that can scale clinically, technically, and regulatorily simultaneously. Teams that solve this early move faster later.
Mindbowser’s Proven Development Process
Most telemedicine urgent care platforms fail for one simple reason. They are built like consumer apps and hardened later like healthcare systems. That sequence breaks under scale and scrutiny.
Mindbowser flips the order. We design urgent care platforms as regulated healthcare infrastructure from day one, then layer speed on top. The process is repeatable, auditable, and tuned for Series B realities where time, capital, and credibility all matter.
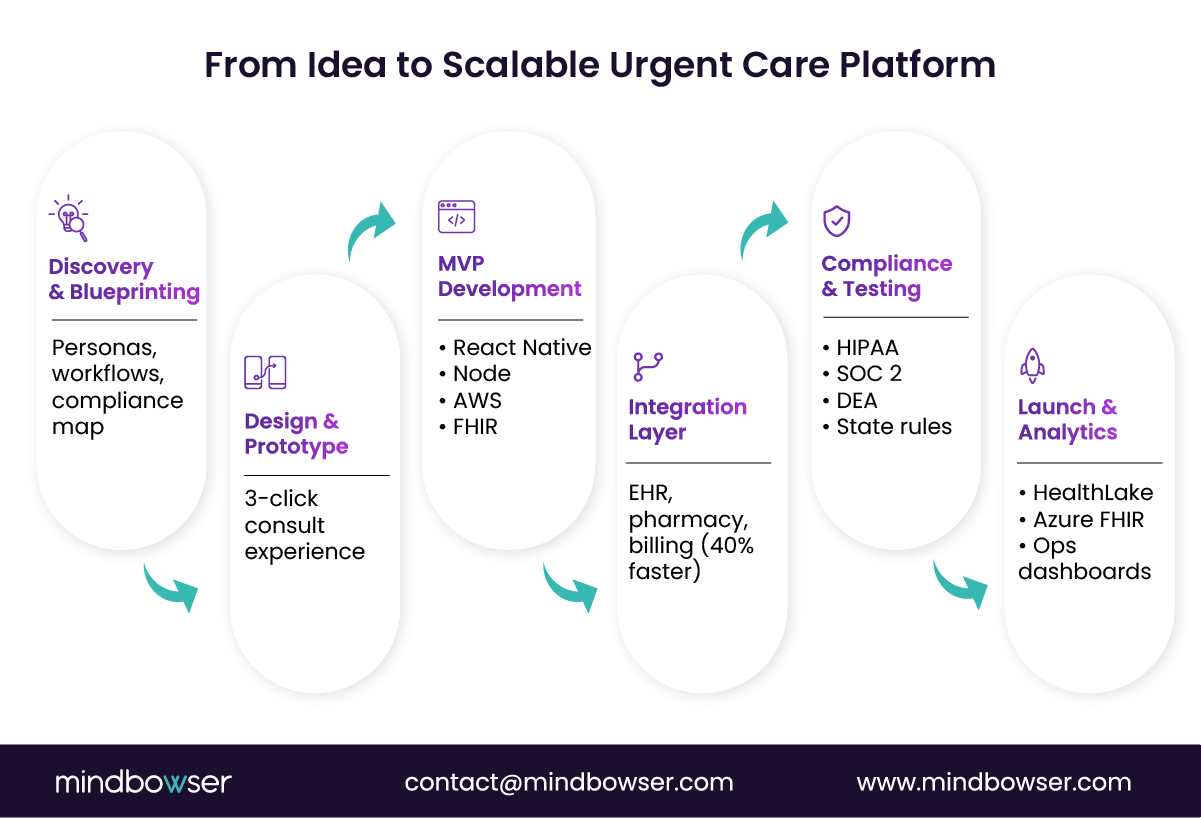
1. Discovery and Blueprinting
This phase sets the ceiling for everything that follows.
We start by mapping:
- Patient personas and visit intent patterns
- Clinician workflows by state and licensure
- Regulatory requirements tied to care types and geographies
- MVP scope aligned to revenue and launch milestones
Instead of generic requirements documents, teams leave with a system blueprint that defines data models, integration points, and compliance boundaries. This is where most downstream rework is eliminated.
2. Design and Prototype
Urgent care UX is about decisiveness. Every extra click increases abandonment.
Our design phase focuses on:
- A three-click consult flow from symptom entry to provider connection
- Clear handoffs between patient, clinician, and system automation
- Edge case handling for dropped calls, incomplete intake, or prescription blockers
Interactive prototypes surface failure modes early, before engineering time is spent.
3. MVP Development
The core platform is built using proven, healthcare-ready stacks:
- React Native for consistent mobile experiences
- Node.js services are designed around event-driven workflows.
- AWS infrastructure aligned with HIPAA requirements
- FHIR first data models to support future interoperability
Security, logging, and access control are implemented alongside features, not bolted on later.
4. Integration Layer
This is where many startups slow down.
Mindbowser’s Healthcare Interoperability Accelerator standardizes:
- EHR and FHIR resource mapping
- Auth and consent flows
- Data normalization across partners
The result is up to 40 percent faster integration timelines compared to building each connector from scratch, without sacrificing flexibility.
5. Compliance and Testing
Before launch, platforms undergo structured validation for:
- HIPAA safeguards and audit readiness
- SOC 2 Type II controls aligned to investor expectations
- DEA-compliant ePrescribing workflows
- State-specific telemedicine requirements
This phase reduces surprises during enterprise sales and diligence.
6. Launch and Analytics
We deploy with observability baked in.
Using tools like AWS HealthLake or Azure FHIR services, teams gain real-time insight into:
- Visit volume and throughput
- No-show and abandonment rates
- Clinical outcomes tied to workflows
Mindbowser’s process is designed to help Series B startups move fast without creating future drag. It turns telemedicine urgent care from a product feature into a durable platform.
Key Features for High-Performing Platforms
At scale, telemedicine urgent care stops being about “having features” and starts being about how those features work together under pressure. High-performing platforms are opinionated. They remove clinician friction, reduce patient uncertainty, and surface operational signals in real time.
Below are the core capabilities that separate durable platforms from fragile ones.
AI-driven Symptom Triage
Urgent care lives and dies on routing accuracy.
Modern platforms use AI triage to:
- Collect structured symptom data before the visit
- Route patients to the right clinician or care pathway
- Flag red-risk scenarios for escalation
The payoff is twofold. Clinicians spend less time gathering basics, and patients enter visits with clearer expectations. Over time, triage data becomes a powerful asset for staffing forecasts and care optimization.
Low-latency WebRTC Video
Video quality is non-negotiable in urgent care.
High-performing platforms invest in:
- WebRTC configurations tuned for healthcare environments
- Intelligent bandwidth adaptation across mobile and desktop
- Session resilience for reconnects and device switching
With properly architected infrastructure, WebRTC can support 15,000 concurrent HD sessions without degradation, even during peak demand. This is not default behavior. It requires deliberate system design.
Secure Messaging and ePrescribing
Not every interaction belongs on video.
Asynchronous messaging supports:
- Follow-up questions
- Lab result clarification
- Prescription coordination
Integrated, DEA-compliant ePrescribing enables clinicians to act immediately during visits while maintaining full audit trails. This reduces leakage to external tools and keeps the care loop closed.
Billing and Claims Integration
Revenue friction kills adoption.
Top platforms embed:
- Eligibility checks during intake
- Automated CPT and ICD coding
- Claims submission and reconciliation
- Consumer payment flows for self-pay models
When billing logic lives inside the platform, no-shows drop and collections improve.
EHR and FHIR Interoperability Modules
FHIR is only useful when it is flexible.
High-performing systems expose modular integration layers that allow teams to:
- Persist only clinically relevant data
- Normalize records across multiple EHR partners
- Extend workflows without rewriting integrations
With FHIR R4 covering 87 percent of EHR needs, custom control becomes a force multiplier, not a cost center.
Patient NPS and Outcomes Analytics
Urgent care generates rich signals quickly.
Platforms that win long-term track:
- Visit completion and abandonment
- Time to resolution
- Repeat usage and satisfaction
- Clinical outcomes tied to protocols
These insights guide product decisions and strengthen payer conversations.
Features do not win markets. Systems do. The right feature set, built as a cohesive platform, turns telemedicine urgent care into a repeatable growth engine.
Get a Custom Telemedicine Urgent Care Roadmap
Mindbowser’s Telemedicine Expertise
When startups reach Series B, buyers, investors, and enterprise partners stop asking what you built and start asking who built it and how repeatable it is. This is where execution history matters more than slideware.
Mindbowser’s telemedicine experience is grounded in building regulated systems that survive scale, audits, and real-world clinical use.
Case Study 1:
An organization needed to move fast without fragmenting care delivery. Their challenge was not the video. It was orchestration.
Mindbowser delivered a custom telemedicine urgent care platform that:
- Integrated directly with the client’s EHR using FHIR-based workflows
- Embedded payment and eligibility checks inside the visit flow
- Reduced clinician context switching across tools
The result was faster visit completion, fewer billing errors, and a platform that could expand into employer and payer contracts without re-architecture.
Case Study 2:
A client approached urgent care from a continuity angle. They wanted to extend virtual urgent care beyond the visit.
Mindbowser implemented:
- AI-driven remote monitoring logic layered on top of urgent care visits
- Automated follow-ups tied to clinical risk signals
- Secure messaging workflows that reduced unnecessary repeat visits
This allowed them to convert urgent care encounters into longitudinal engagement without adding clinician load.
What Differentiates Mindbowser
Across engagements, several patterns hold.
- 50+ healthcare platforms delivered, spanning telemedicine, RPM, urgent care, and value-based care
- Proven delivery under HIPAA, GDPR, HL7, and DEA-aligned requirements
- Deep experience with SOC 2 Type II preparation and audit support
- 30 to 40 percent development time reduction through accelerators, without sacrificing customization
Importantly, Mindbowser does not sell platforms. We build them.
Clients retain:
- Full IP ownership
- Control over data models and workflows
- Freedom to evolve the product post-launch
Why This Matters to Series B Teams
At this stage, engineering teams are already stretched—compliance questions slow sales cycles. Integration debt slows roadmap velocity. Every wrong build decision compounds.
Mindbowser’s role is to reduce that risk, not by abstracting complexity away, but by absorbing it upfront with healthcare-native patterns that have already been proven in production.
Telemedicine urgent care success depends on execution under constraint. Mindbowser brings pattern recognition, regulatory fluency, and delivery muscle so Series B startups can scale with confidence.
Cost and Timeline Snapshot
For Series B startups, the fear around custom telemedicine urgent care development is rarely a capability. It is predictability. CTOs want to know two things upfront: how long it will take and what it will really cost.
When built with healthcare-native frameworks and accelerators, custom does not mean open-ended.
Typical Development Phases
A well-scoped telemedicine urgent care platform follows a clear progression. Each phase has a purpose and a bounded outcome.
| Phase | Timeline | Estimated Cost |
| Discovery & Blueprinting | 3–4 weeks | $15K–$25K |
| UX Design & Prototyping | 2–3 weeks | $20K–$35K |
| MVP Development | 8–10 weeks | $80K–$120K |
| Integrations & Compliance | 4–6 weeks | $40K–$70K |
| Launch & Optimization | 2–3 weeks | $15K–$30K |
Total timeline: ~4–5 months
Typical investment range: $170K–$280K, depending on scope and integrations
This structure assumes reuse of proven video, FHIR, and compliance components rather than greenfield experimentation.
Where the Money Actually Goes
Understanding cost drivers helps prevent scope creep.
- Compliance and security engineering
HIPAA safeguards, SOC 2 controls, audit logging, and role-based access are not optional. They account for a meaningful portion of early spend, but they eliminate downstream rewrites. - Integration complexity
Each EHR, pharmacy, or billing partner adds variability. Platforms that plan for integration extensibility upfront avoid exponential cost growth later. - Real-time infrastructure
Video, messaging, and analytics pipelines require a cloud architecture that can absorb sudden spikes without degradation.
Why Does Custom Cost Less Over Time
White-label platforms appear cheaper initially, but costs rise with scale:
- Per-visit and per-provider fees compound
- Custom workflows trigger paid vendor customizations
- Compliance gaps create rework during diligence
By contrast, NEJM data shows custom telemedicine platforms return 3.8x ROI within 24 months, nearly double that of white-label solutions. The savings come from margin control, reduced no-shows, and faster iteration.
Predictable cost plus controlled upside beats low upfront pricing with hidden ceilings. Custom telemedicine urgent care development becomes financially safer as usage grows.
Scaling Beyond MVP
Shipping the MVP is not the hard part. Staying ahead after product market fit is.
Once telemedicine urgent care proves demand, usage patterns change fast. Visit volumes spike, payer conversations deepen, and clinical leaders ask for more intelligence from the platform. This is where architectural decisions made early either pay off or slow everything down.
High-growth teams treat the MVP as a foundation, not a finish line.
AI-driven triage and predictive analytics
As visit volume increases, manual routing becomes a bottleneck.
Advanced platforms layer predictive models on top of triage data to:
- Anticipate visit surges by geography and season
- Optimize clinician staffing in real time
- Flag patients likely to re-present within 72 hours
Because urgent care generates structured, repeatable data, these models improve quickly. The result is lower wait times, higher clinician utilization, and better outcomes without adding headcount.
Agentic AI for Documentation and Coding
Documentation is one of the highest hidden costs in urgent care.
Next-stage platforms deploy agentic AI to:
- Draft clinical notes during the encounter
- Suggest ICD and CPT codes based on visit context
- Reduce after-visit documentation time for clinicians
The impact is not just speed. It is clinician retention. Reducing cognitive load directly improves satisfaction and lowers turnover in high-volume care settings.
Conversational Bots for Intake and Scheduling
Asynchronous interaction becomes critical at scale.
Well-designed bots handle:
- Symptom intake before visits
- Scheduling and rescheduling
- Status updates during wait times
This reduces the front desk workload and improves patient confidence, especially during peak demand periods. Importantly, these bots are tightly integrated with clinical workflows, not generic chat overlays.
Real-Time Operational Dashboards
Executives need visibility beyond visit counts.
Mature telemedicine urgent care platforms expose dashboards that track:
- Time to provider connection
- Abandonment and no-show rates
- Visit duration and resolution metrics
- Revenue per visit by cohort
These insights inform staffing, pricing, and expansion decisions. Without them, growth becomes reactive instead of intentional.
Why Custom Platforms Scale Cleaner
Every capability above depends on access to clean, owned data and flexible workflows. Platforms built on white-label tools struggle here. Custom platforms evolve without waiting on vendor roadmaps.
Scaling beyond MVP is about intelligence, not features. Custom telemedicine urgent care platforms give startups the data and control required to grow without chaos.
Owning the Future of Telemedicine Urgent Care
Telemedicine urgent care is no longer a tactical add-on—it’s a strategic growth platform. For Series B digital health startups, the real question isn’t speed to launch, but whether your infrastructure can withstand rising demand, regulatory scrutiny, and operational complexity at the same time.
White-label tools help validate demand, but they rarely sustain long-term differentiation or control. Over time, integration friction, compliance retrofits, shrinking margins, and roadmap misalignment create constraints that slow growth. Custom platforms reverse that pattern by enabling full ownership of clinical and operational data, purpose-built workflows that reduce no-shows and clinician burden, compliance built in from day one, scalable video and analytics infrastructure, and expansion into longitudinal, employer, or payer-driven models.
The financial case reinforces the strategic one. Custom platforms demonstrate significantly stronger ROI within 24 months compared to white-label solutions, alongside measurable improvements in no-shows and ER diversion. For growth-stage teams, investing in the right foundation accelerates scale. Mindbowser supports this transition—helping Series B companies move beyond MVPs to enterprise-grade, compliant, and fully owned telemedicine urgent care platforms built for long-term growth.
Telemedicine urgent care platforms often surface licensure complexity earlier than traditional care models. Because visits may originate across state lines, platforms must support real-time provider eligibility checks, state-specific license tracking, and visit routing based on the scope of practice. Startups that ignore this early often face delayed launches in new states or compliance-driven throttling of growth.
Yes, but only if the platform is designed with flexible identity, billing, and reporting layers. Employer-sponsored urgent care requires eligibility verification, employer-level reporting, and, in some cases, different visit flows than those in direct-to-consumer models. Platforms that hard-code assumptions early struggle to serve both without duplication.
Malpractice exposure does not disappear in virtual care. It shifts. Risk is influenced by documentation quality, protocol adherence, and escalation pathways. Platforms that embed clinical decision support, standardized documentation, and clear handoff rules tend to reduce ambiguity, which is often a bigger driver of risk than visit modality itself.
Urgent care telemedicine data can strengthen payer conversations when platforms capture resolution rates, ER diversion metrics, and time-to-care data. Startups that can demonstrate reduced downstream costs gain leverage in value-based discussions, especially when urgent care is positioned as a front door rather than a standalone service.
Earlier than most teams expect. Even if international rollout is not on the immediate roadmap, early decisions around data residency, consent models, and identity management can either enable or block future expansion. Platforms built with global considerations avoid costly re-architecture when new markets become strategic.


