



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 


























TL;DR
- Rural healthcare faces persistent access gaps driven by distance, workforce shortages, and unstable connectivity. Telehealth in rural areas only works when platforms are engineered for low bandwidth, fragmented systems, and real patient behavior, not ideal conditions.
- A custom, cloud-native telehealth platform solves this by combining low-connectivity optimization, deep EHR integration, and patient-first UX that drives adoption without increasing clinician burden.
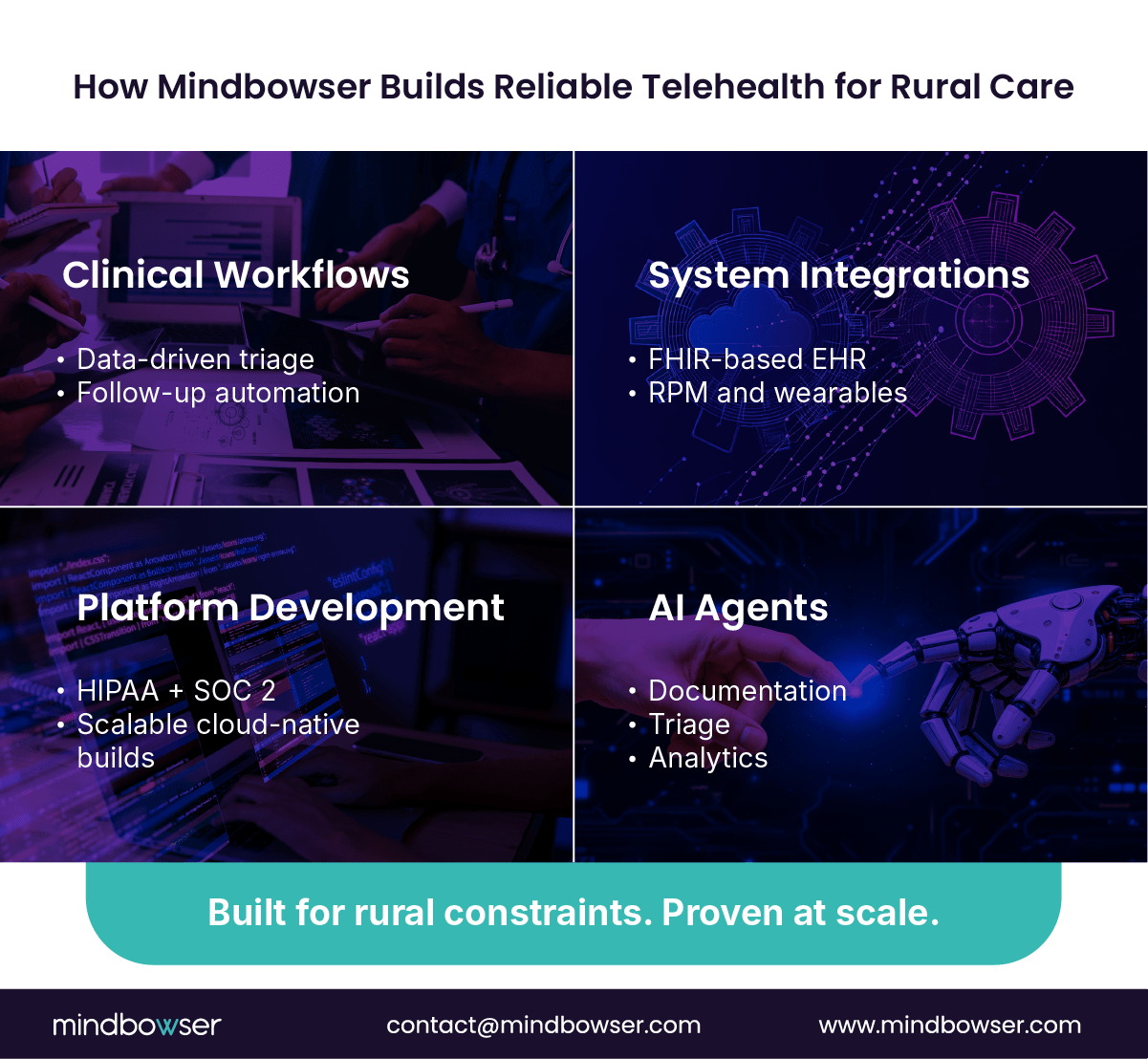
- Mindbowser builds rural-ready telehealth using four proven pillars: Clinical Workflows, System Integrations, Platform Development, and AI Agents.
Why Is Telehealth Critical for Rural Healthcare?
Telehealth in rural areas exists to fix a math problem that bricks-and-mortar care cannot solve.
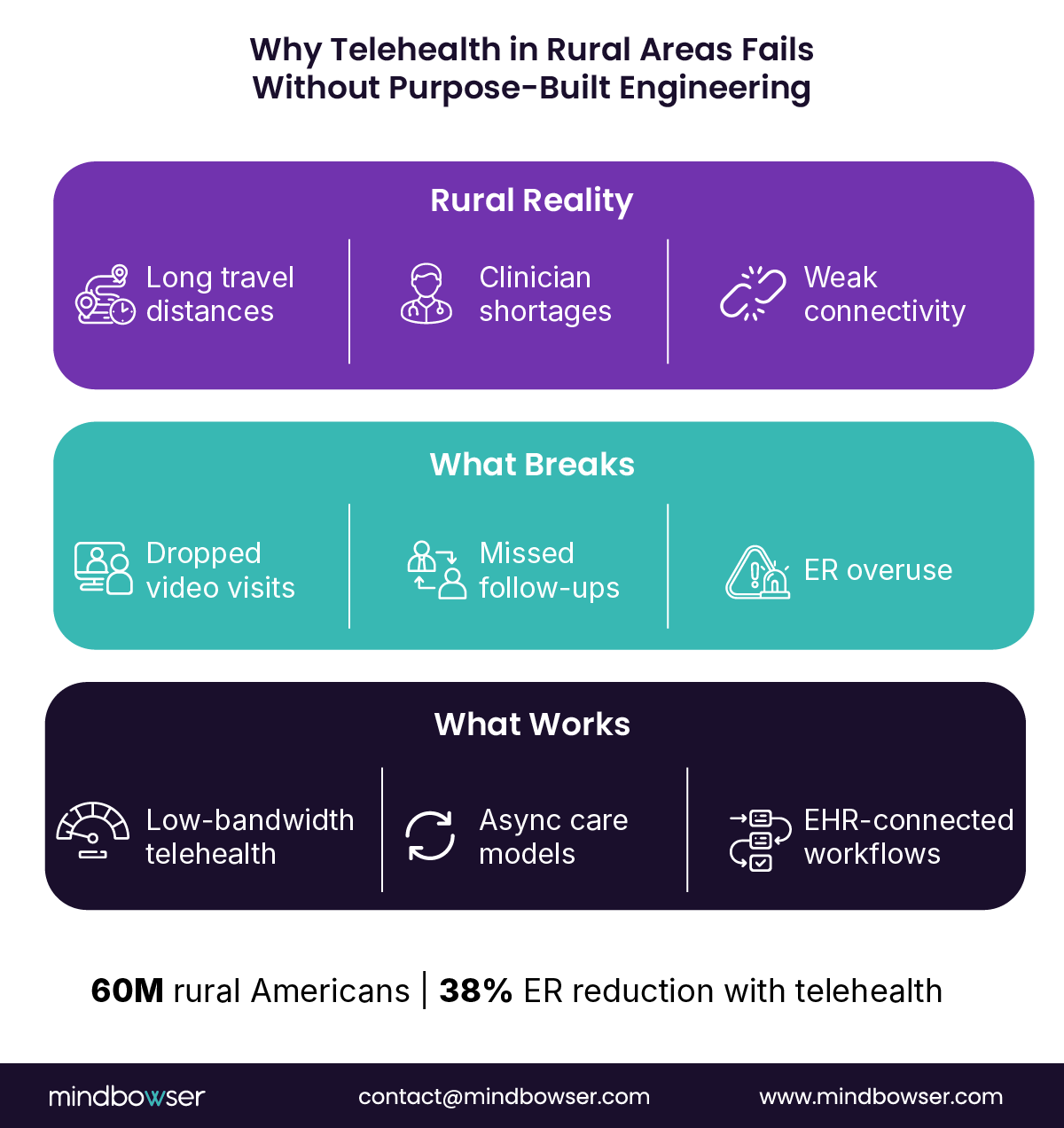
More than 60 million Americans live in rural communities, and over half are medically underserved, with persistent shortages across primary care, behavioral health, and specialty services [HRSA/GAO 2025]. In practical terms, that means fewer clinicians per capita, longer wait times, and care delayed until conditions worsen. Roughly 40 percent of rural residents still lack reliable access to telehealth, even after the pandemic proved demand at scale [HRSA/GAO 2025].
Distance compounds the issue. Rural patients often travel hours for routine visits. The direct and indirect costs land between $500 and $1,200 per patient per trip, once transportation, missed work, and caregiver time are factored in. When access breaks down, emergency rooms become the fallback. That is expensive for health systems and disruptive for patients.
Well-designed telehealth changes this dynamic. Federal evaluations show that mature rural telehealth programs reduce ER utilization by 38 percent, lower avoidable readmissions, and improve follow-up adherence. This is not a theoretical ROI. It is operational relief.
COVID accelerated adoption, but speed masked structural flaws. Many platforms launched quickly without accounting for rural bandwidth limits, EHR fragmentation, or licensing complexity. As emergency waivers sunset, sustainability now depends on engineering discipline, not policy tailwinds.
Telehealth is critical to rural healthcare because it restores access, reduces unnecessary acute care, and stabilizes costs. But it only delivers value when the platform is built with rural constraints in mind from day one.
What Unique Challenges Do Developers Face?
Building telehealth in rural areas breaks most urban-first assumptions. The constraints are structural, predictable, and unforgiving. CTOs who plan for them upfront scale faster. Those who do not spend quarters refactoring.
A. Connectivity and Infrastructure
Rural connectivity is inconsistent by design, not by exception.
Roughly 64 percent of rural households rely on 3G or 4G networks, with average speeds between 15 and 25 Mbps and frequent latency drops during peak hours [FCC/Ookla 2025]. Fixed broadband is often unavailable or unreliable. Video-first telehealth stacks fail here, quietly at first, then catastrophically.
The fix is architectural. WebRTC can deliver functional video at roughly 200 Kbps. When paired with adaptive bitrate controls and audio-first fallbacks, platforms can achieve up to 70 percent bandwidth savings versus traditional video pipelines [FCC/Ookla 2025].
High-performing rural platforms assume degradation will happen. They design it.
• 3G fallback modes with audio prioritization
• Edge caching for visit context, care plans, and consent forms
• Offline data capture with deferred sync
• Store-and-forward workflows for async consults and diagnostics
Progressive Web Apps outperform native apps in these environments. They load faster, tolerate network drops, and reduce update friction. This works. Period.
Reliability in rural telehealth is less about uptime and more about graceful failure.
B. Device and User Constraints
Rural adoption fails when platforms confuse capability with intent.
Patients skew older, manage multiple conditions, and often share devices within households. Many rely on low-cost Android phones with limited storage and older operating systems. Literacy levels vary. Expecting app-store installs, complex sign-ups, or multi-step authentication kills usage.
Mobile-first is table stakes. Mobile for rural is different.
Effective platforms use:
• Large tap targets and simplified navigation
• Plain-language instructions with visual cues
• Voice prompts for visit flow and reminders
• Adaptive streaming that downgrades video before dropping sessions
Adoption does not hinge on features. It hinges on whether the first visit can be done without help.
C. Compliance and Licensing
Scale introduces legal drag.
Today, 27 states require separate provider licenses for telehealth delivery, complicating multi-state expansion and provider scheduling models [FSMB 2025]. On top of that, HIPAA compliance and SOC 2 controls are mandatory, not differentiators, for any platform handling protected health data at scale [HHS 2025].
The technical impact is real.
• Role-based access must align with state licensure
• Audit trails must survive offline sync scenarios
• Encryption, logging, and retention policies must work across environments
Platforms that bolt on compliance later slow down product velocity and increase risk. Teams that embed it into architecture move faster with fewer surprises.
Rural telehealth fails when compliance is treated as paperwork instead of code.
How to Architect Scalable Rural Telehealth
Scalability in rural telehealth is not about handling peak traffic. It is about surviving bad conditions without breaking care delivery. The architecture has to absorb connectivity loss, EHR fragmentation, and compliance controls while still shipping features on a predictable roadmap.
A. System Architecture Blueprint
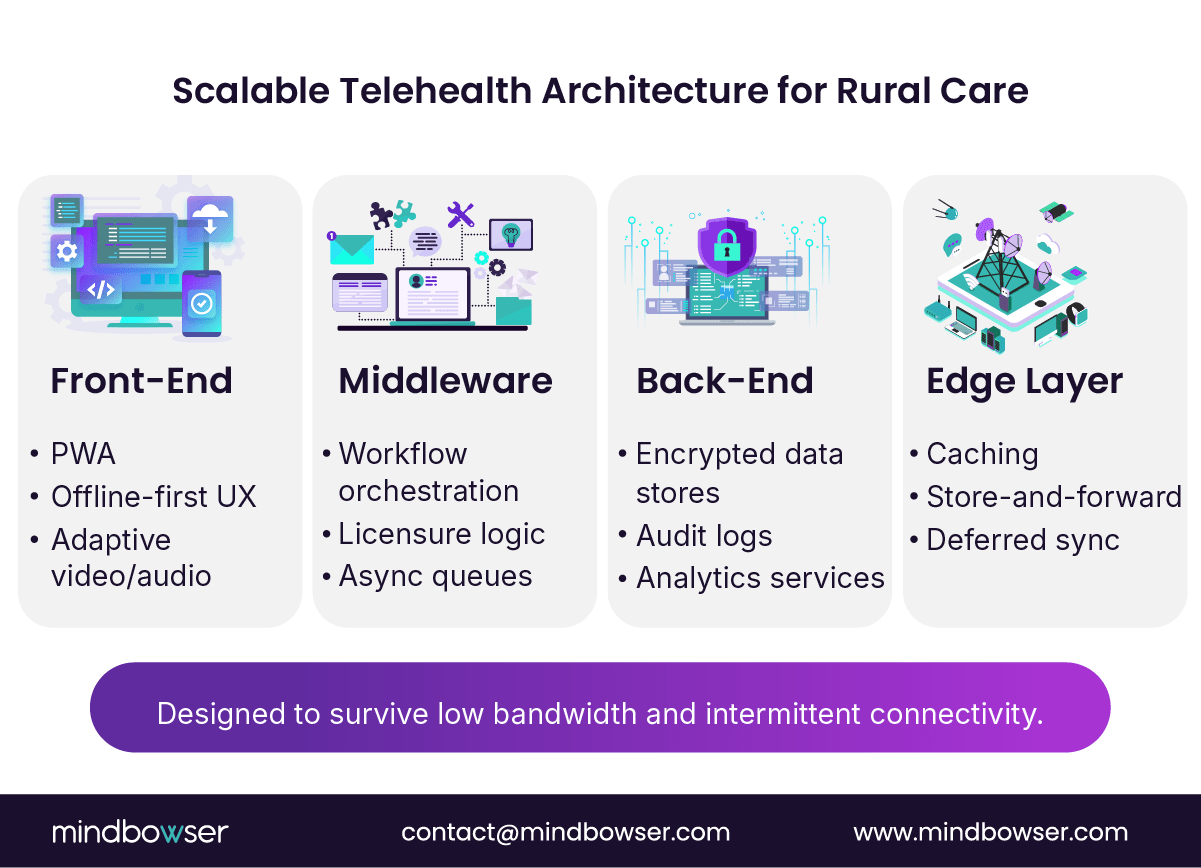
The fastest way to fail in rural environments is to treat architecture as a monolith. High-performing platforms separate concerns across layers and push resilience as close to the edge as possible.
This separation lets teams tune performance where it matters most. When connectivity drops, the edge and front-end carry the experience. When volume spikes, the back-end scales independently.
Rural scalability comes from isolation, not consolidation.
B. Technology Stack
The stack must balance performance, security, and operational cost. Fancy tooling does not help if it fails on a weak signal.
A proven rural-ready stack includes:
• WebRTC or Agora for low-bandwidth video and audio sessions
• AWS S3 and DynamoDB for encrypted, highly available storage with predictable latency
• AES-256 encryption with zero-trust access controls across all services
• Kubernetes-based orchestration for controlled scaling and environment parity
• Power BI or Looker for population and operational dashboards that matter to executives
This approach keeps infrastructure elastic without sacrificing control. More importantly, it lets teams quantify ROI, not just uptime.
C. EHR and RPM Integration
Integration is where most rural telehealth platforms stall.
Rural hospitals use heterogeneous EHR systems, often with partial implementations and custom workflows. Hard-coded integrations do not scale. FHIR-based interoperability layers do.
FHIR bridges normalize patient data, scheduling, and clinical documentation across systems while insulating the core platform from vendor churn. When paired with IoMT gateways, remote patient monitoring data flows asynchronously, tolerating bandwidth drops without losing clinical context.
This matters because rural connectivity constraints are real. With WebRTC operating at roughly 200 Kbps and delivering up to 70 percent bandwidth savings, platforms can prioritize critical signals while deferring non-essential data sync [FCC/Ookla 2025].
Scalable rural telehealth depends less on the EHR brand and more on how cleanly you abstract it.
Mindbowser’s Four Engineering Strengths
Most telehealth platforms claim flexibility. Rural healthcare exposes whether that flexibility is real. Mindbowser’s approach is grounded in four engineering strengths built specifically for environments where bandwidth is thin, workflows are fragmented, and ROI scrutiny is constant.
1. Clinical Workflows
Rural care fails when workflows mirror urban assumptions.
Mindbowser designs data-driven clinical workflows that reflect how rural care is actually delivered. Triage logic prioritizes acuity when specialist access is limited. Follow-up pathways account for delayed connectivity. Care plans adapt based on visit completion, not calendar schedules.
These workflows reduce clinician load while improving outcomes. Automated routing ensures the right provider sees the right patient at the right time, even across state lines and care settings. The result is fewer handoffs, higher-quality documentation, and measurable improvements in follow-up adherence.
Workflow design is the fastest lever for clinical and financial impact.
2. System Integrations
Integration debt kills scale.
Mindbowser uses FHIR-based interoperability layers to connect EHRs, labs, pharmacies, and remote patient monitoring devices without hard-coded dependencies. This allows platforms to absorb new health system partners and device vendors without rewriting core services.
Wearables and IoMT data flow through secure gateways built for asynchronous ingestion. When connectivity drops, data queues locally and syncs once the signal returns. No data loss. No manual reconciliation.
This approach matters in rural environments where EHR maturity varies widely. Integration becomes an asset, not a blocker.
3. Platform Development
Security and scale are designed in, not audited later.
Mindbowser builds HIPAA- and SOC 2–aligned platforms by default, embedding encryption, access controls, and audit logging into every service layer. Kubernetes-based infrastructure supports predictable scaling while maintaining parity across development, staging, and production environments.
Custom builds matter here. Clients retain full IP ownership and avoid vendor lock-in, while accelerators compress time-to-market without compromising architectural discipline. Platforms launch faster and age better.
Compliance-first engineering reduces friction as platforms grow.
4. AI Agents
Manual workflows do not scale in rural care.
Mindbowser deploys AI agents to automate clinical documentation, intake triage, and population-level analytics. These agents operate within defined guardrails, reducing administrative time while preserving clinician oversight.
The impact is tangible. Fewer clicks per visit. Faster documentation. Cleaner data for reporting and ROI tracking. This is how platforms reduce cost per encounter without cutting care quality.
AI works when it removes work that clinicians never wanted to do.
Start Building Your Rural Telehealth Platform Today
Development Strategies for Reliability
Reliability in rural telehealth is earned during development, not recovered in production. Platforms that succeed under weak connectivity, regulatory pressure, and scale constraints share the same engineering discipline.
A. Agile and DevSecOps
Speed without control breaks healthcare platforms.
Rural telehealth teams need Agile delivery paired with DevSecOps, with security and compliance checks running in the pipeline, not after release. Continuous integration and deployment pipelines enforce HIPAA validation, automated testing, and configuration drift detection on every build.
Kubernetes plays a central role. It standardizes environments, supports rolling updates, and allows teams to isolate failures without taking down the platform. More importantly, it enables predictable scaling as usage grows across regions and service lines.
The result is faster iteration without increasing risk. CTOs get velocity. Compliance teams get audit-ready systems.
Bottom line. Reliability improves when every release is production-ready by default.
B. Low-Connectivity Testing
Most telehealth platforms fail because they are never tested in real rural conditions.
Mindbowser teams simulate 2G and 3G network environments during QA to observe how applications behave under packet loss, latency spikes, and dropped connections. Deferred sync logic, offline form submission, and retry mechanisms are validated before launch.
This testing discipline prevents the most common rural failure mode: silent data loss. Visits that appear completed but never reach the EHR erode clinician trust quickly. Once trust is lost, adoption follows.
Reliable platforms prove themselves when networks fail.
If it does not survive 3G, it does not belong in rural care.
C. Localization and Access
Adoption depends on relevance.
Rural populations are linguistically and culturally diverse. Platforms that support regional languages, simplified medical terminology, and SMS-based onboarding see higher engagement and lower drop-off rates. SMS matters because it works on every phone, with or without data plans.
Localization also extends to workflows. Appointment reminders, care instructions, and follow-up messages must align with how patients actually live and work. Technology that respects context drives sustained usage.
Reliability includes being understood, not just being online.
Data Security and Patient Trust
In rural telehealth, trust is the platform.
Patients are being asked to share sensitive data over unstable networks, often on shared devices. Clinicians are being asked to rely on systems that must withstand regulatory scrutiny. If security feels bolted on, adoption stalls.
Effective telehealth in rural areas starts with end-to-end encryption across every data path. All data in transit and at rest must be encrypted using industry standards, including AES-256, with keys managed under strict access controls. This protects patient information even when sessions drop or data sync is deferred.
Identity management is equally critical. Multi-factor authentication, role-based access, and least-privilege policies ensure that only authorized users access protected health information. In multi-region deployments, identity logic must also respect licensure boundaries and care team roles.
Verification adds another layer of confidence. Platforms that support SSN-based or national ID validation, where appropriate, reduce fraud and ensure accurate patient matching across fragmented systems. This becomes essential as platforms scale across states and care settings.
Finally, audit readiness cannot be optional. Continuous logging, immutable audit trails, and real-time monitoring allow teams to demonstrate compliance at any moment, not just during annual reviews. For CTOs, this reduces operational drag. For patients, it signals seriousness.
Bottom line. Security is not just about compliance. It is about earning the right to be trusted with care.
What’s Next for Rural Telehealth
The future of telehealth in rural areas will be determined less by features and more by the discipline of infrastructure. The winners will design for uneven progress, not perfect conditions.
1. Connectivity Will Improve, But Never Evenly
Rural broadband will not flip overnight.
What’s changing:
• 5G expansion across secondary and tertiary markets
• Low-earth-orbit satellite networks reaching remote regions
• Incremental gains, not uniform coverage
What stays true:
• Dead zones persist
• Latency spikes remain common
• Bandwidth varies by hour, not just location
Design implication: Platforms must continue to treat low-bandwidth modes as first-class citizens, with higher-fidelity experiences layered on top when connectivity allows.
Bottom line. Assume variability forever.
2. Edge AI Will Outpace Centralized Intelligence
Cloud-only intelligence struggles in rural environments.
What’s emerging instead:
• Edge AI models that run closer to patients and clinicians
• Local symptom triage and risk flagging
• Priority routing when connectivity returns
Why this matters:
• Faster response under weak signals
• Less dependency on continuous cloud access
• Preservation of clinical signal during outages
Design implication: Intelligence moves closer to care delivery, not farther away.
3. Federated Learning Will Shape Population Health
Rural systems care deeply about privacy and data control.
Federated learning enables:
• Model improvement without moving raw patient data
• Cross-population insights without centralizing PHI
• Alignment with HIPAA-first architectures
For CTOs, this means:
• Lower data exposure risk
• Easier multi-partner collaboration
• Better longitudinal insight without heavier pipelines
Design implication: Learn together. Store separately.
4. Blockchain Portability Will Gain Relevance
Still early. Increasingly relevant.
Why it matters in rural care:
• Patients receive care across geographies and systems
• Records fragments over time and distance
• State lines complicate continuity
Blockchain-based portability offers:
• Patient-controlled longitudinal records
• Durable identity across providers
• Reduced dependency on bilateral integrations
Design implication: Portability shifts from vendor-driven to patient-driven.
The next generation of rural telehealth platforms will win by prioritizing resilience first, intelligence second, and polish last.
How Mindbowser Builds for Rural
Mindbowser does not retrofit urban telehealth platforms for rural use. We engineer for rural constraints from day one, where connectivity breaks, workflows fragment, and ROI scrutiny is relentless.
Proven Impact in Rural and Underserved Settings
What happens when platforms are built correctly:
• 35 percent lift in follow-up compliance, driven by low-bandwidth UX and async workflows
• Fewer missed visits due to offline-first scheduling and SMS reminders
• Cleaner documentation with less clinician effort
These outcomes align with industry benchmarks showing 3.2x ROI within 18 months, 45 percent reductions in hospital admissions, and 22 minutes saved per visit when telehealth platforms are engineered for reliability and automation [NEJM/HIMSS 2025].
Bottom line. Results appear in utilization, not in slide decks.
What Makes Mindbowser Different
- Bandwidth-Aware Engineering Frameworks
• Audio-first and adaptive video pipelines
• Offline data capture with deferred sync
• Store-and-forward baked into care delivery - Compliance Toolkits Built Into the Stack
• HIPAA and SOC 2 controls embedded at every layer
• Continuous audit readiness, not annual fire drills
• Role- and licensure-aware access control - Population Health and ROI Dashboards
• Real-time visibility into utilization and outcomes
• Executive-ready metrics tied to cost reduction
• Actionable insights, not raw data exports
This combination allows CTOs and product leaders to scale across regions without rewriting platforms or compromising trust.
Building Scalable and Reliable Telehealth Platforms for Rural Care
Building telehealth in rural areas is not just a UX problem; it’s an engineering challenge with significant clinical, regulatory, and financial consequences. Platforms must be designed to respect rural constraints, or they will fail under pressure. Mindbowser’s approach works because it’s engineered to thrive in these conditions.
Mindbowser’s strategy begins with clinical workflows tailored to rural realities, such as limited specialists, delayed follow-ups, and variable connectivity. By designing workflows that account for these factors, care continues even when systems encounter issues. Additionally, system integrations are crucial, and Mindbowser uses FHIR-based interoperability to connect EHRs, devices, and data sources without relying on brittle, one-off integrations.
The approach also includes platform development that ensures HIPAA- and SOC 2-aligned platforms, built to scale predictably, tolerate failures, and provide clients full ownership of their technology and IP. Finally, AI agents automate critical tasks like documentation, triage, and analytics, reducing clinician workload and providing clear ROI. This four-point strategy enables telehealth platforms to progress from pilot to production, turning good intentions into measurable outcomes.
Reimbursement varies by payer and state, but most rural programs rely on a mix of Medicare, Medicaid, and value-based contracts. Fee-for-service parity has improved since COVID, but long-term sustainability comes from aligning telehealth with chronic care management, remote patient monitoring, and population health incentives. Platforms should be built to support billing codes, documentation standards, and reporting without manual workarounds.
Timelines depend on integration depth and compliance scope, not just features. A basic pilot can launch in 8 to 12 weeks, while enterprise-grade rural platforms with EHR integration, licensure logic, and security controls typically require 4 to 6 months. Teams that use accelerators while maintaining custom architecture move faster without accumulating technical debt.
Technology is rarely the biggest blocker. Change fatigue is. Common challenges include clinician skepticism, workflow disruption, and lack of operational ownership. Successful programs invest early in clinician training, align telehealth workflows with existing care models, and assign clear accountability for adoption metrics. Platforms must reduce clicks, not add steps, to gain trust.
Vendor lock-in usually comes from proprietary data models and closed integrations. Platforms built on open standards like FHIR, modular services, and cloud-native infrastructure allow health systems to switch vendors, add partners, or expand use cases without replatforming. Full IP ownership and transparent architecture matter more than feature lists.
Uptime and visit counts are table stakes. Executive teams should track:
- Follow-up compliance rates
• ER diversion and admission reduction
• Cost per encounter over time
• Clinician time saved per visit
• Patient retention across care episodes
These metrics tie telehealth performance directly to financial and clinical outcomes, not just usage.


