



















 BLOGS
BLOGS  NEWSROOM
NEWSROOM  CASE STUDIES
CASE STUDIES  WEBINARS
WEBINARS  PODCASTS
PODCASTS  ASSET HUB
ASSET HUB  EVENT CALENDAR
EVENT CALENDAR 

























TL;DR:
CCM + APCM – 2026 CMS Rates (Non-Facility)
Standard CCM
- 99490 (first 20 min): $66.13/month
- 99439 (each +20 min): $50.44/month
- 99491 (first 30 min): $89.18/month
- 99437 (each +30 min): $63.13/month
- 99487 (first 60 min): $144.29/month
- 99489 (each +30 min): $78.16/month
- G0556 Basic (0-1 conditions): $16.37/month
- G0557 Expanded (2+ conditions): $53.78/month
- G0558 Advanced (2+ conditions + social complexity): $117.24/month
This guide breaks down every CCM CPT variant, including staff-time, physician-time, and complex CCM, and shows how time thresholds, supervision, and medical decision-making determine which code applies. Real claims examples highlight where payers pay cleanly and where they push back, especially around concurrency with TCM, RPM, and RTM.
For CFOs, the takeaway is clear. CCM remains a predictable recurring revenue stream, but only when add-on minutes are consistently captured and high-acuity patients are coded correctly. For CTOs, CCM is a systems problem. Eligibility checks, consent, time tracking, and concurrency rules must live inside EHR logic, not staff memory.
The G0511 transition for RHCs and FQHCs completed on September 30, 2025. These facilities now bill individual CCM CPT codes (99490, 99439, 99487, 99489) the same way as other providers. Any clinic still defaulting to G0511 in 2026 is producing denials and potential recoupment exposure. The guide below covers the correct CPT mapping for each common RHC/FQHC scenario.
While CCM remains time-based in 2026, leaders must also evaluate the growing role of Advanced Primary Care Management (APCM) codes (G0556–G0558). Unlike CCM, APCM shifts reimbursement from minute tracking to bundled monthly payments tied to care continuity. High-performing organizations are now segmenting patients, keeping high-touch cohorts in CCM while moving stable populations to APCM for operational simplicity and predictable revenue.
Are you confident your CCM program is using the right CPT code mix in 2026, or are you quietly leaking $66.30 to $117-$134 per patient per month while increasing audit risk?
Chronic Care Management remains one of the most predictable reimbursement streams in value-based care. But predictability only holds when coding precision matches CMS rules. In 2026, the CCM code set is stable, yet payment rates, RHC/FQHC timelines, and concurrency enforcement make small operational errors expensive. Pick the wrong code lane, miss a time threshold, or overlap CCM with TCM, and finance sees denials while compliance sees exposure.
For CFOs and CTOs, the problem is not a lack of awareness. It is execution. Coding teams must distinguish between staff-time CCM, physician-time CCM, and complex CCM. Technology teams must ensure the EHR captures time, consent, care plans, and supervision requirements without relying on staff memory. Miss either layer, and you lose revenue or face post-payment clawbacks.
This guide breaks down the 2026 CCM codes in plain terms. It compares every CPT variant, shows how real claims are adjudicated, and provides a practical selection algorithm you can embed directly into workflows. We also quantify updated 2026 revenue math and clarify the extended RHC/FQHC transition deadline, so leadership teams can forecast accurately and stay audit-ready.
I. 2026 CCM CPT Codes at a Glance
If you’re here for the codes and rates only, the table below covers every CCM CPT variant for 2026 – what each code pays, who can bill it, the time threshold, and the single most important documentation requirement for each. Deeper coverage on rules, claims examples, and code selection follows below.
| Code | Description | Time Threshold | Who Bills | 2026 Rate (Non-Facility) | Key Documentation Requirement |
| 99490 | Standard CCM, initial period | 20 min/month | Clinical staff under general supervision | $66.13 | Consent, care plan in CEHRT, time log connected to care activity |
| 99439 | Standard CCM, add-on | Each additional 20 min | Clinical staff under general supervision | $50.44 | Same as 99490 + supplementary minute attribution |
| 99491 | Physician/QHP CCM, initial | 30 min/month | Physician or QHP personally | $89.18 | Provider time documented separately from staff time |
| 99437 | Physician/QHP CCM, add-on | Each additional 30 min | Physician or QHP personally | $63.13 | Same as 99491 + add-on time attribution |
| 99487 | Complex CCM, initial | 60 min/month | Clinical staff under general supervision | $144.29 | Moderate or high MDM explicitly documented |
| 99489 | Complex CCM, add-on | Each additional 30 min | Clinical staff under general supervision | $78.16 | Same as 99487 + supplementary minute attribution |
| G0506 | Initiating-visit care planning add-on | One-time | Billing provider personally | $66.47 | Comprehensive care plan + CCM consent at initiating visit |
| G0556 | APCM Basic | No minute tracking | Practice level (bundled) | $16.37 | 0-1 chronic conditions documented |
| G0557 | APCM Expanded | No minute tracking | Practice level (bundled) | $53.78 | 2+ chronic conditions documented |
| G0558 | APCM Advanced | No minute tracking | Practice level (bundled) | $117.24 | 2+ conditions + social complexity documented |
| G0568 | APCM CoCM Initial (NEW 2026) | No minute tracking | BHI-trained team | ~$162 | Initial collaborative care management – behavioral health |
| G0569 | APCM CoCM Subsequent (NEW 2026) | No minute tracking | BHI-trained team | ~$146 | Subsequent collaborative care management |
| G0570 | APCM General BHI (NEW 2026) | No minute tracking | BHI-trained team | ~$58 | General behavioral health integration |
Three things to notice:
1. The single most-billed code in CCM is 99490 at $66.13/month – that’s the floor. Practices that consistently bill the 99439 add-on add another $50.44/month per qualifying patient, which compounds fast across a 200-patient panel.
2. APCM (G0556-G0558) removes the minute-tracking burden but caps the per-patient ceiling. The decision between traditional CCM and APCM comes down to documentation discipline, not patient mix.
3. The APCM behavioral health add-ons (G0568-G0570) are new for 2026; most billing references haven’t caught up yet. If your panel includes patients with co-occurring depression, anxiety, or substance use disorders, these codes stack on top of APCM and add $58 to $162/patient/month with no minute tracking.
For practices new to CCM coding, start with 99490 + 99439. For practices with disciplined documentation already, layer in 99487 / 99489 for complex patients. For practices with weak documentation systems, evaluate APCM.
Rates verified against CMS 2026 PFS Final Rule (CMS-1832-F) via MedFeeSchedule national non-facility amounts, last verified 2026-04-14.
The table above covers every active CCM and APCM code for CY 2026. The cheat sheet below is a 1-page printable version, with all codes, rates, time thresholds, supervision rules, and documentation requirements in one place. Billers keep it open during claims review.
What’s on the cheat sheet:
- CPT 99490, 99439, 99487, 99489, 99491 – rates, time, who bills
- APCM codes G0556/G0557/G0558 + 2026 behavioral health add-ons (GPCM1, GPCM2, GPCM3)
- Concurrency rules (what can stack, what can’t)
- Supervision requirements by provider type
- Top 3 denial triggers + how to avoid them
Access The 2026 CCM And APCM Cheat Sheet To Simplify Claims Review And Avoid Common Billing Errors.
Our team has helped hospital networks and digital health startups design scalable, compliant CCM workflows that cut audit risk and drive measurable growth.
II. What Is CPT Code 99490? Standard CCM, Explained
CPT 99490 is the entry-point billing code for non-complex Chronic Care Management. It’s also the most frequently billed CCM code in the country and the one most often left under-billed because practices stop at the base 20-minute threshold without capturing add-on time.
Definition
CPT 99490 covers the first 20 minutes per calendar month of clinical staff time spent on chronic care management for a patient with two or more chronic conditions, delivered under the general supervision of a physician or qualified health professional. It’s the standard, non-complex CCM code – the one most CCM programs are built around.
What 99490 actually pays
At 2026 non-facility rates: $66.13 per patient per month, or roughly $793.56 per patient per year at base billing without add-ons. Add-on time (99439, +20-minute increments) layers another $50.44 per increment on top.
Who can bill it
99490 is billed by the supervising physician or qualified health professional (QHP). The clinical staff member doing the work – typically an RN, LPN, or experienced medical assistant- does not personally bill the code; the supervising provider does. Only one practitioner may bill 99490 per patient per month.
Eligible billing providers: MD, DO, NP, PA, CNS, or CNM.
Time threshold
The 20-minute threshold is cumulative across the calendar month, not per-encounter. A 5-minute call on the 8th, a 7-minute medication reconciliation on the 14th, and an 11-minute follow-up call on the 26th all add up to 23 minutes – which clears the threshold and qualifies the patient for 99490 that month. Each documented activity must connect to the care plan; idle wall-clock minutes don’t count.
Required documentation
Every 99490 claim must be backed by:
1. Patient consent – verbal is acceptable under current rules, written is preferred for audit defense. Must be dated and obtained before any CCM time is logged.
2. Active care plan stored in certified EHR – not a Word document, not an uploaded PDF. Structured EHR data.
3. Time log – start/stop times or activity duration, attributed to the staff member performing the work, tied to a specific care plan element.
4. 24/7 access protocol – patient must have a documented way to reach the care team round-the-clock; this can be the practice’s main line with an after-hours protocol.
5. Initiating visit – annual wellness visit, comprehensive E/M, or TCM visit must precede the first CCM month, and consent + care plan must originate from that encounter.
What goes wrong with 99490 most often
- Under-billing the 99439 add-on. Most practices document 25-35 minutes of activity but only bill 99490, leaving the 99439 ($50.44) unbilled. A 200-patient panel that captures the add-on for 60% of patients picks up ~$72,500/year in revenue that was already worked.
- Concurrency overlap with TCM. If a 99495/99496 (TCM) was billed for the patient in the past 30 days, 99490 cannot overlap – CCM time has to start after day 30 of the post-discharge window.
- Initiating visit missing. First CCM claim without a documented initiating visit triggers automatic denial. Every patient needs the upstream encounter on file before CCM time begins.
- Free-text care plans. A care plan in a Word document or note field, rather than as structured CarePlan data in the EHR, fails certified-EHR requirements and exposes claims to recoupment.
99490 vs other CCM codes
- 99490 vs 99491 – 99491 is the same idea, but for time delivered personally by the physician or QHP, not by clinical staff. 99491 pays more ($89.18) but staff minutes don’t count toward it.
- 99490 vs 99487 – 99487 is complex CCM. Time threshold is 60 minutes (vs 20 for 99490) AND moderate-to-high MDM must be documented. 99487 pays $144.29 but is harder to defend in audit.
- 99490 vs APCM (G0556-G0558) – APCM removes minute tracking entirely. Use APCM if your documentation systems are weak or if you want predictable monthly revenue without the time-log overhead.
For most practices, 99490 + 99439 is the bread and butter of CCM revenue. The other codes layer on top for specific patient profiles.
III. CCM in 2026: What Changed and What Didn’t
A. CCM vs Complex CCM vs Physician-Time CCM
Chronic Care Management still operates in three clearly defined lanes. The codes are unchanged. The risk comes from choosing the wrong one.
- Non-complex CCM (99490, 99439)
This is staff-driven care management. Clinical staff provide at least 20 minutes per month under general supervision. It remains the most common CCM entry point and the most frequently undercoded when add-on time is not captured. - Complex CCM (99487, 99489)
This lane applies when staff provide 60 minutes or more, and the care requires moderate to high medical decision-making. For a deeper breakdown, see our guide to complex chronic care management. - Physician or QHP-time CCM (99491, 99437)
These codes apply when the physician or qualified health professional personally performs the care management work. Staff minutes do not count. These codes carry a higher value but also higher scrutiny, because payers expect clear proof of provider involvement.
Time, complexity, and who delivered the care matter equally. If any one of those elements is misclassified, the claim fails.
From a systems design perspective, this classification is not just clinical- it must be encoded into workflow logic. Modern implementations use rule engines inside EHR middleware to automatically route patients into the correct CCM lane based on time logged, provider involvement, and documented complexity. Without this, organizations rely on manual judgment, which is where most miscoding originates.
B. 2026 Policy Rules That Still Drive Code Choice
While CMS did not introduce new CCM codes for 2026, enforcement around existing rules remains strict.
- Concurrency rules
1. Non-complex CCM and complex CCM cannot be billed for the same patient in the same month.
2. CCM and TCM may only be billed together if their service periods do not overlap.
3. CCM may be combined with either remote patient monitoring or RTM, but not both at the same time. - Initiating visit requirement
Before the first CCM claim, the patient must have an annual wellness visit, a comprehensive E/M visit, or a TCM visit. Consent and a documented care plan must originate from this encounter. - G0506 add-on
When the billing provider personally performs extensive care planning at the initiating visit, G0506 may be billed. It remains optional, but valuable for complex patients.
Most CCM denials are not about eligibility. They are about overlapping dates, missing consent, or insufficient documentation tied to the initiating visit.
One nuance that continues to create confusion is the interplay with Principal Care Management (PCM) and APCM. While PCM remains mutually exclusive with CCM, APCM introduces a parallel pathway. Systems must now evaluate not only concurrency conflicts but also strategic eligibility, deciding which reimbursement model yields better outcomes for a given patient cohort.
C. New for 2026: APCM Behavioral Health Add-On Codes
CMS introduced three behavioral health add-on G-codes that pair with APCM for 2026, expanding APCM’s reimbursement scope for practices managing patients with co-occurring chronic and behavioral health conditions. None of these require minute-based tracking, which is the operational point – they’re billable on documented complexity, not stopwatch time.
| Code | Use Case | 2026 Rate | Equivalent CoCM/BHI Code |
| G0568 | Initial Collaborative Care Management – behavioral health | ~$162/month | Functionally similar to 99492 |
| G0569 | Subsequent Collaborative Care Management – behavioral health | ~$146/month | Functionally similar to 99493 |
| G0570 | General Behavioral Health Integration | ~$58/month | Functionally similar to 99484 |
When to use:
- G0568 / G0569 apply when a practice runs a Collaborative Care Management model with a behavioral health care manager and a psychiatric consultant. G0568 is the first month a patient enrolls in CoCM; G0569 covers subsequent months.
- G0570 applies when a practice provides general behavioral health integration without the full CoCM model – useful for primary care practices that have an embedded behavioral health clinician but not a structured CoCM program.
Stacking rules:
- These codes pair with APCM (G0556-G0558) and add to the per-patient revenue
- They do NOT pair with traditional CCM (99490-series) – APCM-only stack
- A patient cannot have both G0568 and G0569 in the same month (they’re sequential by definition)
- Documentation requires a behavioral health diagnosis and evidence of integrated care (consultation notes, referral records, treatment plan elements)
Why this matters for revenue modeling:
A practice running APCM Advanced (G0558 at $117.24) for a patient with depression and substance use disorder can stack G0568 in the first month ($162) and G0569 in subsequent months ($146). That’s a per-patient/month total of approximately $263–$279 for a high-complexity APCM patient with behavioral health comorbidity – substantially above any single CCM code and competitive with complex CCM (99487 + 99489) without minute-tracking burden.
For practices serving dual-eligible populations or panels with high SDOH burden, the APCM + behavioral health stack is the most overlooked revenue lever in the 2026 fee schedule.
Note on rate accuracy: G0568, G0569, G0570 rates above are national averages from industry sources (DLA Piper analysis + Nsight Health + EHR Source 2026 guidance). Final 2026 PFS final rule rates may vary by ±2-5% by MAC region. Verify against your MAC fee schedule before forecasting at scale.
Code naming verification (added 2026-05-02): The internal Page 1 audit referenced these codes as “GPCM1 / GPCM2 / GPCM3” – that’s a different code family (used for the Shared Savings Program, not APCM). The correct codes for APCM behavioral health add-ons are G0568, G0569, G0570 as drafted above. Verified across CMS-aligned industry sources.
D. RHC/FQHC Update for 2026 (Deadline Extended)
The G0511 transition completed September 30, 2025. RHCs and FQHCs now bill individual CCM CPT codes the same way as other provider types – there is no “extended” deadline.
What this means in 2026:
- G0511 should not appear on any 2026 claim. Claims submitted with G0511 after September 30, 2025 are denied automatically.
- Use individual CCM CPT codes: 99490 (initial 20 min), 99439 (each additional 20 min), 99487 (complex initial 60 min), 99489 (complex add-on 30 min). Same code rules as any other practice.
- APCM is also available for RHCs and FQHCs as of 2025 – G0556, G0557, G0558. The complexity-based bundled payment model often suits the patient profile in rural and safety-net settings better than minute-tracking CCM.
- Documentation requirements remain identical to other settings: consent, care plan in CEHRT, time logs, MDM evidence for complex CCM.
What to do if you’re still defaulting to G0511 in 2026:
If your billing system or coder still uses G0511, fix the workflow before the next billing cycle. Submitted G0511 claims are auto-denied and do not auto-correct to the right CPT – they need to be re-submitted under the right code. Each month of delay is a month of zero RHC/FQHC chronic-care revenue, not a delayed payment.
The clinics that prepared early in 2025 are seeing 15-25% revenue uplift over the old G0511 flat rate because individual CPT billing rewards documented time and complexity. The revenue is there for any clinic that fixes the billing setup.
E. APCM Behavioral Health Add-On Codes (2026 Update)
In addition to standard APCM bundles (G0556–G0558), CMS has introduced behavioral health add-on codes that expand reimbursement opportunities for integrated care models.
Codes:
- GPCM1
- GPCM2
- GPCM3
These codes apply when behavioral health services are layered onto longitudinal primary care management, particularly for patients with mental health or substance use conditions.
Coding accuracy alone is not enough; documentation must support every billed minute. Our CCM audit risk and protection guide explains how to avoid audit failures.
IV. Side-by-Side CCM CPT Codes
Time • Supervision • Who Can Bill • Documentation Keys
For CTOs and CFOs, this section is the control panel. Every denial, audit request, or revenue shortfall usually traces back to one of these distinctions being missed in workflow design.
Operationally, the biggest gap we see is not understanding these codes-it is failing to capture structured time logs. High-performing systems embed timers, activity tagging, and automated attribution into workflows so that every minute is defensible at audit time.
A. Non-Complex CCM by Clinical Staff
Codes: 99490 (first 20 minutes), 99439 (each additional 20 minutes)
- Time threshold
- Minimum 20 minutes per calendar month for 99490
- Each additional 20-minute increment captured with 99439
- Time must be cumulative and tied to care management activities
- Supervision
- General supervision
- Billing provider oversees care but does not need to be present
- Who can bill
- MD, DO, NP, PA, CNS, or CNM
- Only one practitioner per patient per month
- Documentation keys
- Active care plan maintained in a certified EHR
- Patient consent documented
- Detailed staff time logs linked to care activities
- Evidence of 24/7 access to clinical staff
Finance note: This is the most common CCM code family and the most under-monetized. Missed 99439 add-ons quietly erode margins at scale.
B. Physician or QHP-Time CCM
Codes: 99491 (first 30 minutes), 99437 (each additional 30 minutes)
- Time threshold
Minimum 30 minutes personally performed by the physician or QHP
Staff time does not count - Supervision
Not applicable, since the billing provider performs the service - Who can bill? Only the physician or QHP who personally delivered the care
- Documentation keys
- Explicit provider time tracking
- Notes must reflect direct physician/QHP involvement
- Clear separation from staff-driven activities
- Time threshold
C. Complex CCM by Clinical Staff
- Codes: 99487 (first 60 minutes) and 99489 (each additional 30 minutes).
- Time Requirement: Minimum of 60 minutes of clinical staff time per month. Additional increments of 30 minutes are billed under 99489.
- Supervision Level: General supervision.
- Who Can Bill: MD, DO, NP, PA, CNS, or CNM
- Documentation Keys:
- Moderate or high medical decision-making is explicitly documented
- Coordination among multiple providers
- Medication reconciliation and adherence checks
- Care plan updates reflecting patient complexity
Compliance reality: Time alone does not justify complex CCM. Without documented MDM, these claims fail in review.
D. Initiation and Care-Planning Add-On
Code: G0506.
- When it applies
At the initiating visit, when the billing provider personally performs extensive care planning - Documentation keys
1. Comprehensive care plan details
2. CCM consent captured
3. CEHRT linkage
Strategic use: Optional, but valuable for complex patients where upfront planning time is significant.
E. Programs Commonly Confused With CCM
- Principal Care Management (PCM, 99424–99427)
1. Single chronic condition, expected to last at least three months
2. Not interchangeable with CCM, which requires two or more conditions
- Transitional Care Management (TCM, 99495–99496)
1. Covers the 30-day post-discharge period
2. May be billed in the same month as CCM only if service periods do not overlap
CTO takeaway: These distinctions must live in logic, not training decks. If your EHR cannot enforce them automatically, your revenue depends on memory.
For a detailed breakdown of complex CCM billing and documentation, see our Complex CCM guide (99487/99489).
Your CCM Strategy Deserves More Than Guesswork
Our team has helped hospital networks and digital health startups design scalable, compliant CCM workflows that cut audit risk and drive measurable growth.
V. Real Claims Examples (What Actually Gets Paid in 2026)
Rules look clean on paper. Claims do not. This section shows how CCM CPT codes behave once they hit payer systems and where teams either protect revenue or create risk.
Across multiple implementations, denial patterns consistently trace back to three root causes: unstructured documentation, concurrency overlap, and unclear attribution between staff and provider time. Organizations that address these at the system level, not through training alone, see denial reductions of 50–70%.
A. Family Medicine Example: 99490 + 99439
- Patient Profile: 72-year-old patient with diabetes and congestive heart failure.
- Workflow: A nurse care manager logged 32 minutes across the month. Activities included medication reconciliation, scheduling specialty follow-ups, and weekly outreach calls.
- Claim Submission:
- 99490 for the first 20 minutes
- 99439 for the additional time (rounded to a full 20-minute increment)
- Remittance Outcome: Both line items were paid. Total reimbursement exceeded the base CCM rate.
- Audit Note: Time logs were linked directly to the care plan. The EHR produced a clean activity trail, which is exactly what auditors expect to see.
Why this matters:
Most practices stop at 99490 even when the time exceeds 20 minutes. That hesitation leaves money on the table every month.
B. Complex CCM Example: 99487 + 99489
- Patient Profile: 65-year-old patient with COPD, diabetes, and hypertension.
- Workflow: Clinical staff recorded 92 minutes coordinating care among a pulmonologist, PCP, and pharmacist. Medication changes followed a recent hospitalisation.
- Claim Submission:
- 99487 for the first 60 minutes.
- 99489 for the additional 32 minutes.
- Remittance Outcome: Claim paid in full at complex CCM rates.
- Audit Note: The provider explicitly documented moderate complexity medical decision-making and inter-provider communication. Without that MDM language, the claim would likely have been downgraded or denied.
- Compliance lesson: Time alone does not protect complex CCM claims. Decision-making does.
C. Physician-Time CCM Example: 99491 + 99437
- Patient Profile: 77-year-old patient with advanced Parkinson’s disease requiring frequent medication adjustments.
- Workflow: The physician personally spent 65 minutes across the month managing care, including direct patient calls and care plan revisions.
- Claim Submission:
- 99491 for the first 30 minutes
- 99437 for the additional 35 minutes
- Remittance Outcome: Claim accepted at physician-time rates.
- Audit Note: Documentation clearly separated physician work from staff activities. Staff time was excluded, protecting the claim from recoupment.
- Finance takeaway:
Physician-time CCM supports high-acuity care, but only when time attribution is clean.
D. TCM Handoff to CCM Within the Same Month
- Patient Profile: 68-year-old patient discharged after heart failure exacerbation.
- Workflow:
- TCM services are billed for the first 30 days post-discharge
- CCM activities began after day 30, with 25 minutes logged
- Claim Submission:
- 99495 for TCM
- 99490 for CCM after the TCM period ended
- Remittance Outcome: Both claims were paid.
- Audit Note: The EHR blocked CCM time logging during the TCM window, preventing overlap.
- Risk avoided: Overlapping service dates are one of the fastest ways to trigger denials.
E. RHC/FQHC Transition Example (2026 Timeline Applied)
- Patient Profile: A 70-year-old patient was treated at a rural health clinic.
- Workflow: Clinical staff provided 42 minutes of CCM services.
- Claim Logic:
Through September 30, 2025: G0511 was used for general care management
From October 1, 2025 onward: 99490 + 99439 reflect actual time delivered
In 2026: All RHC/FQHC CCM claims use individual CPT codes – G0511 is no longer accepted - Remittance outcome: Reimbursement remained stable, with improved flexibility once add-on codes were used.
- Operational lesson: Clinics that adapted workflows ahead of the September 2025 deadline are now seeing 15-25% revenue uplift over the old flat G0511 rate. Clinics still defaulting to G0511 in 2026 are eating denials month over month; fixing the billing setup is the highest-ROI fix any RHC/FQHC can make right now.
📌 Key Insight:
In 2026, payers reward precision. Claims fail most often when staff minutes are double-counted, when CCM overlaps with TCM, or when complexity is asserted without decision-making evidence.
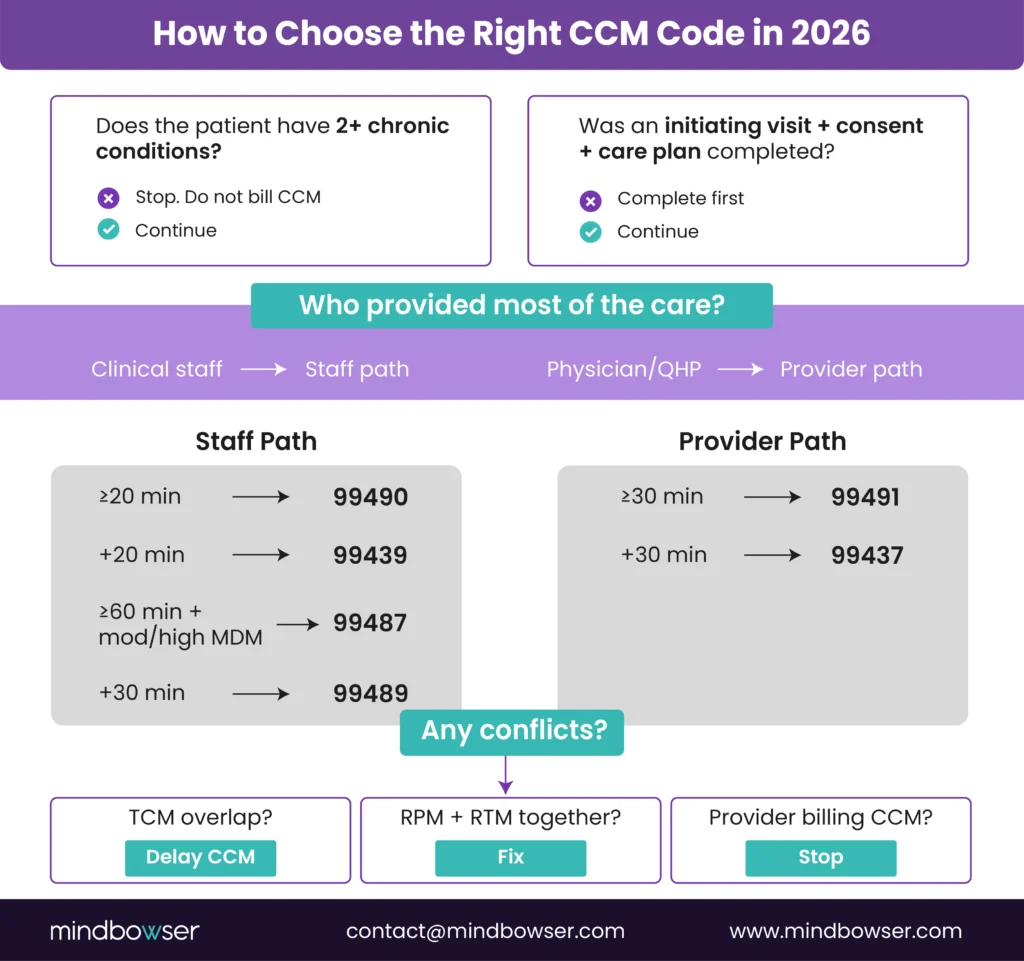
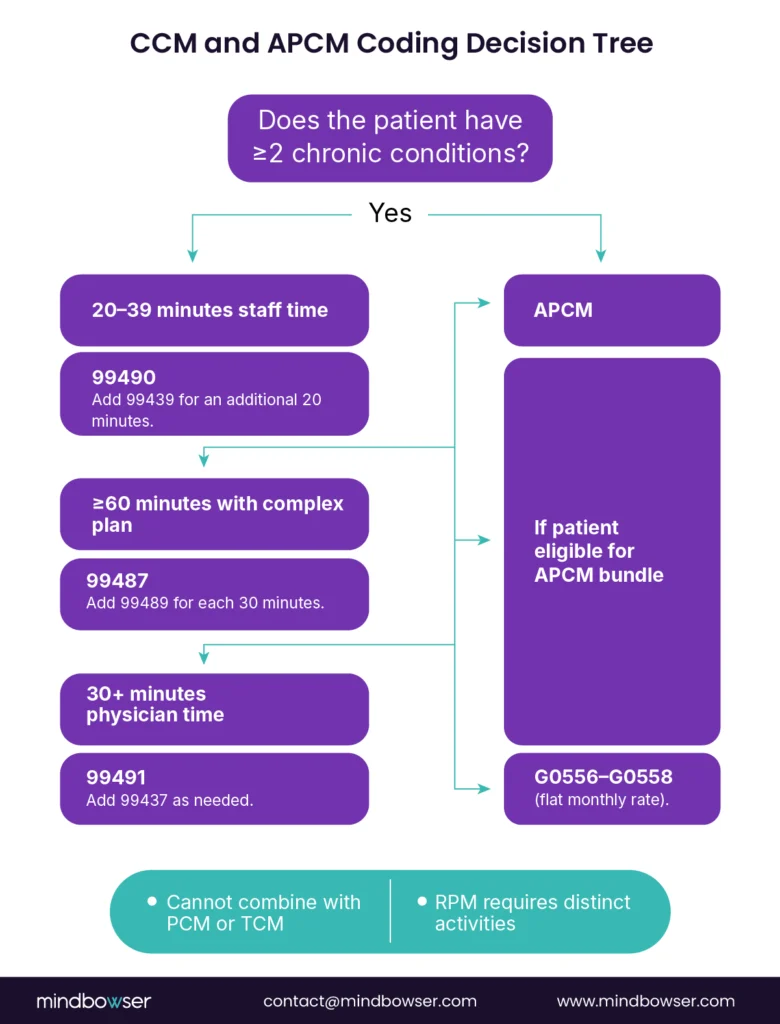
VI. Selecting the Right CCM Code: A Practical 2026 Algorithm
Most CCM errors are not knowledge gaps. They are decision failures at the point of care. This algorithm turns policy into a repeatable process your teams and systems can follow every month.
In advanced implementations, this algorithm is not a checklist; it becomes an automated decision tree embedded in the EHR. Inputs such as ICD-10 conditions, time logs, and encounter types dynamically determine the correct CPT code, eliminating reliance on manual coding decisions.
A. Step 1: Confirm Patient Eligibility and Initiating Visit
Before any CCM time is logged, confirm the foundation is in place.
- The patient has two or more chronic conditions expected to last at least 12 months or until death.
- The conditions place the patient at significant risk of death, acute exacerbation, or functional decline.
- An initiating visit has occurred. This may be an annual wellness visit, a comprehensive E/M visit, or a transitional care management visit.
- Patient consent is documented in the certified EHR.
- A care plan is created and stored in CEHRT.
Control point: If any of these elements are missing, CCM should not be billed. Systems should block time capture until the task is complete.
B. Step 2: Choose the Care Delivery Lane
Once eligibility is confirmed, identify who delivered the majority of the work.
- Staff-Time CCM (99490, 99439): Select this lane when clinical staff perform most of the care management under general supervision.
- Physician/QHP-Time CCM (99491, 99437): Use this lane only when the physician or QHP personally provides at least 30 minutes of care. Staff minutes must be excluded.
- Complex CCM (99487, 99489): Choose this lane when staff provide at least 60 minutes, and the care involves moderate or high medical decision-making
Execution risk: Mixing lanes within the same month leads to denials.
If your teams are still relying on memory to select CCM codes, this is where errors begin. The decision flow below translates CMS rules into a repeatable logic your EHR should enforce.
C. Step 3: Apply Time Thresholds and Add-On Codes
- 99490: First 20 minutes of staff time.
- 99439: Each additional 20 minutes of staff time.
- 99491: First 30 minutes of physician/QHP time
- 99437: Each additional 30 minutes of physician/QHP time
- 99487: First 60 minutes of complex CCM.
- 99489: Each additional 30 minutes of complex CCM.
- G0506: Optional add-on at the initiating visit for extensive provider-led care planning.
If the minimum time threshold is not met, the code should not be billed.
D. Step 4: Check Concurrency and Conflicts
Before finalising the claim, confirm there are no overlaps.
- Non-complex CCM and complex CCM cannot be billed in the same month.
- CCM and TCM may only be billed together if the service periods do not overlap.
- CCM may be paired with either RPM or RTM, but not both.
- Only one practitioner may bill CCM for a patient per month.
System requirements: These checks should be automated, not manual.
E. Step 5: Apply Special Setting Rules (2026)
- Rural Health Clinics and Federally Qualified Health Centers:
1. G0511 transition completed September 30, 2025 – no longer billable
2. Bill individual CCM CPT codes (99490, 99439, 99487, 99489) – same rules as other providers
3. APCM (G0556-G0558) is also available and may suit rural/safety-net patient profiles better than minute-based CCM - Specialty Practices: Principal Care Management may be more appropriate when only one chronic condition is being managed.
F. Output: The Decision Tree
When embedded in an EHR, this logic becomes a decision tree:
- Is the patient eligible and consented?
- Was an initiating visit completed?
- Who delivered the care: staff or provider?
- How much time was logged?
- Any overlapping services?
- Any special setting rules?
Result: The correct CCM CPT code is selected automatically, reducing denials and underbilling.
Stop Losing CCM Revenue to Coding Complexity
Mindbowser helps you translate real-world workflows into automated, audit-ready billing logic inside your EHR – so every minute counts and every claim gets paid.
VII. EHR Prompts That Reduce Errors and Denials (2026 Execution Layer)
Most CCM revenue losses do not result from misunderstanding the rules but from gaps in execution and documentation. Our CCM audit risk and compliance guide breaks down how to avoid common audit failures. It comes from relying on people to remember them. In 2026, high-performing organizations hardwire CCM compliance into the EHR so errors never reach billing.
A. Pre-Billing Guardrails
- Initiating Visit Check
Before any CCM claim is generated, the EHR should confirm that an initiating visit exists. Acceptable encounters include an annual wellness visit, a comprehensive E/M visit, or a TCM visit.- If no initiating visit is on file, the claim submission should be blocked.
- This control alone eliminates one of the most common audit findings.
- Consent Verification
Consent must be documented prior to initiating CCM billing.
- Use a structured consent field tied to the patient record.
- Billing logic should remain locked until consent is captured.
- Certified EHR Documentation
Care plans must live in certified EHR technology.
- Prompts should require documentation of diagnoses, goals, medications, involved providers, and follow-up cadence.
- Free-text care plans increase audit risk.
B. Time and Complexity Controls
- Separate Time Counters”
The EHR should track staff time and physician/QHP time independently.- At 20 minutes, prompt for 99490.
- At 40 minutes, prompt for 99439.
- At 60 minutes with documented MDM, prompt for 99487.
- Physician/QHP time should trigger 99491 only when provider minutes reach 30.
- Complexity Documentation
For complex CCM, time alone is insufficient.
- The system should require explicit documentation of moderate or high medical decision-making.
- Templates should guide providers to document problem complexity, medication changes, and coordination with other clinicians.
Audit protection: If complexity fields are incomplete, the claim should not advance. If complexity fields are incomplete, the claim should not advance.
C. Concurrency Enforcement
- TCM Overlap Alerts
If a TCM claim is active within 30 days of discharge:- CCM time entry should be disabled during the overlap period.
- CCM logging should reopen automatically after day 30.
- RPM and RTM Exclusivity
When remote monitoring codes are active:
- The EHR should prompt users to confirm that CCM is paired with either RPM or RTM, not both.
- Duplicate Practitioner Warnings
If another practitioner has already billed CCM for the patient in the same month:
- The system should flag the conflict before submission.
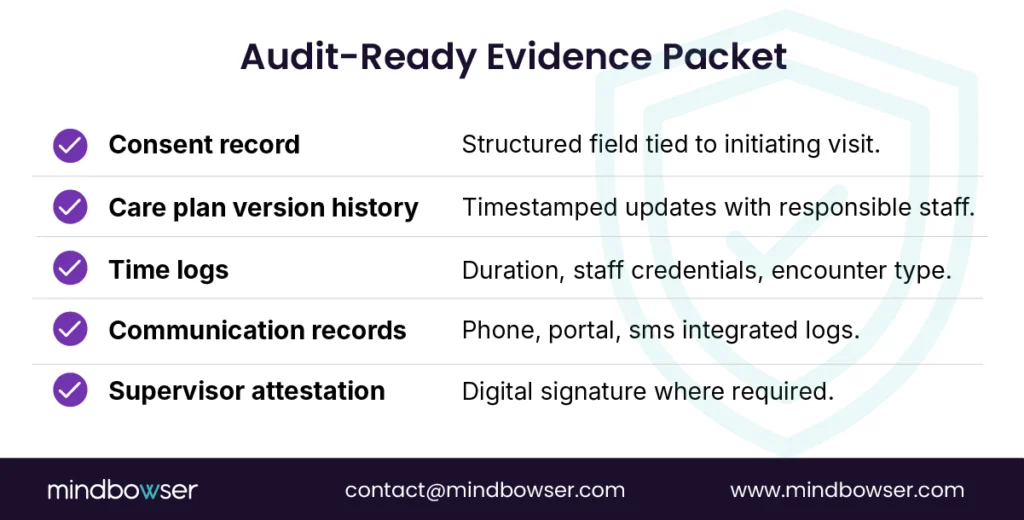
What does an audit-ready CCM program actually need to prove? The checklist below summarizes the minimum evidence CMS and payers expect during reviews.
D. Scaling With Mindbowser Accelerators
Mindbowser operationalizes these controls with accelerators built for CCM scale:
- AI Medical Summary pre-populates care plans from existing records, reducing manual chart review.
- CarePlan AI enforces version control and structured documentation aligned to audit standards.
- RPMCheck AI Validates CCM, RPM, and RTM combinations to prevent concurrency violations.
- HealthConnect CoPilot embeds prompts directly into Epic, Cerner, Athena, and other major EHRs using FHIR and HL7.
All activity logs are immutable and support HIPAA, SOC 2, and 42 CFR Part 2 requirements.
Beyond prompts, leading systems are now adopting FHIR-native architectures where care plans (FHIR CarePlan), tasks (FHIR Task), and audit logs (FHIR AuditEvent, Provenance) are structured and version-controlled. This enables instant audit packet generation and ensures every CCM activity is traceable, queryable, and compliant with USCDI standards.
📌 Key Insight: In 2026, compliance that lives in training decks fails. Compliance that lives in software scales.
VIII. Financial Impact Snapshot for CFOs
For finance leaders, CCM is not a compliance exercise. It is a recurring revenue line within broader value-based care models that lives or dies by code mix discipline and time capture accuracy.
Another overlooked lever is payer variance. While CMS provides baseline rates, commercial payers often diverge significantly. Mature organizations integrate payer-specific fee schedules directly into their financial models, ensuring forecasts reflect real reimbursement rather than national averages.
2026 rate note: The figures below reflect estimated 2026 PFS averages. Final reimbursement varies by geography and payer. CFOs should validate against their MAC fee schedule before forecasting.
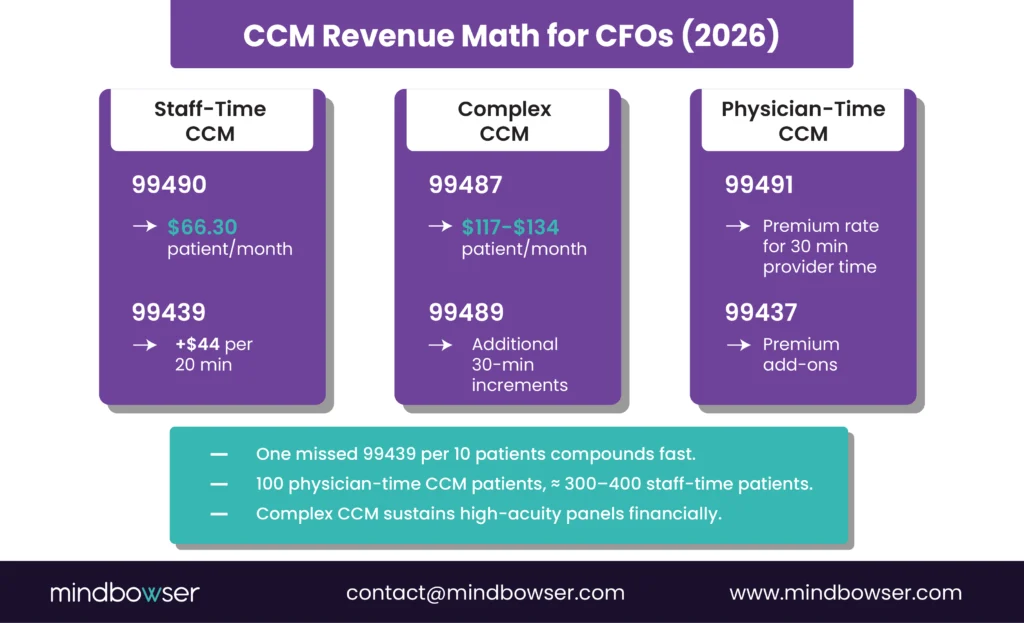
A. Monthly Revenue Ladders by CCM Code Mix
Staff-Time CCM (99490 + 99439)
- 99490: approximately $66.30 per patient per month (2026 est.)
- 99439: approximately $44 per additional 20 minutes (2026 est.)
A panel of 500 eligible patients, with a 40% enrollment rate, can still generate steady monthly revenue at the base threshold. The margin expansion comes from consistency. Capturing even one additional 99439 for every 10 enrolled patients materially changes the annual forecast.
CFO lens: Lost add-on minutes do not show up as denials. They show up as silent underbilling.
Physician-Time CCM (99491 + 99437)
- Higher reimbursement per unit because only the physician’s or QHP time qualifies
- Typically applied to high-acuity panels where provider involvement is unavoidable
In practice, 100 patients billed under physician-time CCM can generate revenue comparable to 300–400 patients billed under staff-time CCM, assuming clean documentation.
Risk tradeoff: These codes pay more, but payer scrutiny is higher. Provider time attribution must be airtight.
Complex CCM (99487 + 99489)
- 99487: approximately $117-$134 for the first 60 minutes (2026 est.) (10% CCM rate increase per CMS Final Rule)
- 99489: additional 30-minute increments, rate stable
Organizations that consistently document moderate or high medical decision-making capture 25–40% more CCM revenue than those defaulting to non-complex CCM for similar patient populations.
Finance reality: Complex CCM is where high-acuity populations become financially sustainable, not where shortcuts are tolerated.
B. RHC/FQHC Transition Economics (2026 Timeline)
- Through September 30, 2026: RHCs and FQHCs may continue using G0511, which pays a flat rate regardless of time or complexity.
- After September 30, 2026: Clinics must bill individual CPT codes such as 99490, 99439, 99487, and 99489.
- Economic Shift:
- G0511 simplifies billing but caps upside.
- Post-transition CPT billing rewards accurate time capture and documentation of complexity.
- Clinics with disciplined workflows can see 15–25% revenue uplift without increasing patient volume.
- Budget implication: Training, EHR reconfiguration, and time-tracking controls are not optional line items in 2026 planning.
C. Staffing Model Tips for Sustainable ROI
- Panel Sizing
- One full-time care manager can typically manage 150–200 non-complex CCM patients.
- Complex CCM lowers panel size but increases per-patient revenue.
- Time Capture Discipline
- Real-time EHR counters prevent missed minutes.
- One extra 99439 per care manager per day compounds into meaningful annual revenue.
- Audit-Ready Documentation
- Consent, care plans, activity logs, and time attribution must support every billed code.
- Recoupments erase margin faster than rate cuts.
📌 Key Insight: In 2026, CCM profitability is not solely driven by enrollment. It is driven by how well time, complexity, and staffing models align with the codes you bill.
IX. Implementation Playbook (First 90 Days, 2026-Ready)
Knowing the codes is table stakes. Execution is where CCM programs either scale cleanly or stall under denials and rework. This playbook outlines how high-performing organizations operationalize CCM in the first 90 days.
Programs that outperform benchmarks typically treat enrollment as a funnel, not a one-time task. By tracking eligibility, outreach, consent capture, and conversion rates, organizations can increase enrollment by 20–25% without expanding patient pools.
A. First 30 Days: Build the Foundation
- Patient Attribution
Start by identifying eligible patients directly from the EHR.- Two or more chronic conditions
- High risk of hospitalization, exacerbation, or functional decline
- Prioritize patients with frequent utilization or recent discharges
Risk stratification here improves both outcomes and revenue yield.
- Consent Capture
Consent failures remain a top audit trigger.- Embed CCM consent prompts into annual wellness visits, TCM visits, and routine E/M encounters
- Store consent in a structured EHR field
- Block billing if consent is missing
- Care Plan Templates
Standardization reduces compliance drift.- Deploy CEHRT-compliant care plan templates
- Require diagnoses, medications, goals, assigned care team, and follow-up cadence
- Avoid free text where possible
- 24/7 Access Protocols
CCM requires around-the-clock access.- Define escalation paths and on-call coverage
- Publish patient-facing contact information
- Reference access details inside the care plan
Leadership checkpoint: By day 30, every enrolled CCM patient should have consent, a care plan, and a documented access pathway.
B. Days 60–90: Optimize and Tune the Code Mix
- Code Mix Review
Compare billed codes against patient acuity.- Are high-risk patients consistently billed under complex or physician-time CCM?
- Are staff-driven patients defaulting to 99490 without add-on capture?
Misalignment here signals lost revenue or elevated audit risk.
- Denials and Near-Misses
Review payer responses weekly.- Common issues include overlapping TCM dates, missing care plans, or weak MDM documentation
- Treat near-miss edits as warnings, not noise
- Documentation Coaching
Targeted training beats broad retraining.- Coach staff on logging activities with precise time stamps
- Train providers to document moderate or high complexity decision-making clearly
- Reinforce that physician-time CCM excludes staff minutes
CTO focus: Use denial patterns to refine EHR prompts and logic, not to add more manual checks.
C. Governance and Compliance Controls
- Role-Based Access
Limit who can log CCM time.
- Separate staff time entry from physician/QHP time entry
- Prevent retroactive edits without justification
- Audit Trails
Every CCM activity should be traceable.
- Who performed the work
- What was done
- How much time was spent
- Which care plan element does it support
Logs should be immutable and exportable for audits.
3. Cross-Functional Oversight
Create a quarterly review cadence.
- Finance reviews revenue trends and leakage
- Compliance reviews documentation sufficiency
- IT reviews workflow friction and system gaps
- Population health reviews outcomes and engagement
Executive takeaway: Programs without governance drift. Drift is where denials and recoupments start.
📌 Key Insight: CCM success in 2026 is not driven by enthusiasm at launch. It is driven by repeatable execution, measured weekly, and enforced by systems.
X. How Mindbowser Helps Teams Execute CCM Without Revenue Leakage
Most organizations do not fail at CCM because they misunderstand the codes. They fail because execution breaks at scale. Mindbowser focuses on the execution layer, where compliance, engineering, and finance intersect. Many organizations implement this through custom chronic care management software built for EHR-native workflows.
In multiple deployments, combining structured workflows with automation has shown measurable impact: enrollment increases of over 20%, denial reductions exceeding 50%, and significant improvements in documentation efficiency. These gains compound over time, turning CCM into a stable revenue engine rather than a compliance burden.
A. Proof Points From the Field
• Remote Patient Monitoring and Elderly Care Platform
Mindbowser built a remote monitoring and care coordination platform for elderly patients with multiple chronic conditions.
1. Achieved 90% patient engagement
2. Delivered twice as fast, reporting for care managers
3. Reduced manual documentation burden while supporting compliant CCM time capture
Why it matters: High engagement and faster workflows translate directly into more defensible CCM minutes.
• Wearable and AI-Driven Risk Detection Platform
For a digital health client, Mindbowser integrated wearable data, EHR connectivity, and predictive alerts into a unified system.
1. Increased patient interaction by 45%
2. Reduced physician review time by 60%
3. Freed staff capacity for documented CCM activities
Why it matters: Automation does not replace CCM. It creates space to bill it correctly.
• AI-Native Health Record for Complex Care
Mindbowser designed an intelligent health record system focused on complex patient populations.
1. Cut documentation time by 70%
2. Accelerated follow-ups by 60%
3. Improved audit readiness for complex CCM claims
Why it matters: Complex CCM only works financially when documentation keeps pace with care delivery.
• Behavioral Health VBC Network
Mindbowser supported a multi-provider behavioral health network connecting hospitals, providers, and payers
1. Reduced readmissions by 52%
2. Lowered Medicaid plan costs by 12.1%
Why it matters: CCM is not just revenue protection. It is a lever for value-based performance.
• Custom Billing-Logic Build – 76% Denial Reduction
A custom care platform built for a maternal-health program embedded billing logic directly into the clinical workflow rather than reconciling claims after the fact. The clinical focus was obstetric, but the billing-automation pattern is identical to what CCM programs need: structured documentation captured at the point of care, claims rules validated before submission, and audit artifacts linked to every billed code.
Outcomes from the billing work:
1. 76% reduction in coding denials
2. ±12-minute prediction accuracy on care plan timing
3. EHR-embedded billing capture at the point of clinical work, eliminating downstream reconciliation
Why this matters for CCM: A 5% denial rate on a $5 million CCM program costs $250,000 a year. Cutting that to 1% recovers $200,000 – enough to fund two coordinators, an EHR upgrade, and still leave margin. The 76% denial reduction on the maternal-health build is the proof that this isn’t a theoretical lever – it’s a workflow design decision that compounds across every code billed.
The same pattern works for CCM: validate eligibility, consent, care plan, and time threshold before the claim is generated, not after. Every concurrency check, every MDM documentation requirement, every initiating-visit reference – caught at the moment the staff member would otherwise commit the error. Denial rate drops because the upstream conditions for denial are blocked before they reach the claims system.
B. Accelerators Built for CCM Compliance
The pattern across CCM-adjacent builds is consistent: programs that capture the full revenue stack do it by treating CCM as a workflow design problem, not a software install. Pre-built components shave 6 to 9 months off custom builds and let the team focus on the workflow design rather than the integration plumbing.
For CCM specifically, the components that matter most:
- CarePlan AI handles the structured care-plan generation that satisfies CEHRT requirements without forcing clinicians to type the same data twice
- HealthConnect CoPilot is the FHIR-native EHR integration layer – the connection between clinical workflow and billing system that closes denial gaps before claims are submitted
- RPMCheck AI validates CCM time-tracking against any concurrent RPM or RTM activity, catching the most common concurrency violation before it reaches a claim
What stays custom: payer-specific billing rules, multi-specialty workflow logic, your specific EHR’s quirks, and the parts of CCM compliance that require defensible audit artifacts unique to your practice’s documentation patterns.
What stays human: the SDOH conversation, consent capture for patients with limited English or cognitive limitations, end-of-life planning discussions, and clinical escalation calls. These don’t automate and shouldn’t – naming them honestly is what separates a credible implementation pattern from a software pitch.
The economic case is straightforward: a CCM program that captures 80% of eligible minutes, holds denials below 2%, and stays audit-clean generates predictable monthly revenue at 250-400% ROI on the coordinator investment. The same program with weak documentation discipline runs at 40-55% capture and barely breaks even. The gap between those two outcomes is workflow design, not licenses.
C. Strategic Advantage for CFOs and CTOs
For CFOs
- Predictable recurring CCM revenue
- Fewer denials and recoupments
- Clear linkage between staffing costs and reimbursement
For CTOs
- Logic-driven workflows instead of manual policing
- EHR-native integrations without rip-and-replace
- Audit trails that satisfy compliance without slowing teams down
Shared benefit: CCM that scales without increasing operational risk.
D. Engagement Models
Mindbowser supports organizations at different stages of CCM maturity.
- Full-Service CCM Build – End-to-end platforms including CCM, RPM, and billing workflows
- Workflow Retrofit – Targeted integrations that add guardrails to existing EHRs
- Performance-Based Partnerships – Revenue-aligned models tied to outcomes and realized reimbursement.
📌 Key Insight: Mindbowser does not just explain CCM rules. We engineer them into systems so revenue is captured correctly every month.
XI. CCM Codes: When Coding Rules Become System Rules
Chronic Care Management in is no longer about learning new CPT codes. It is about executing the existing ones with discipline. The difference between billing 99490 versus 99487, or choosing 99491 over staff-time CCM, is not academic. It directly determines whether revenue is realized, denied, or later recouped.
For CFOs, CCM represents one of the few recurring revenue streams that scales without increasing patient volume. But that only holds when time is captured accurately, add-on codes are applied consistently, and documentation stands up to audit. Underbilling quietly erodes margins. Overbilling invites clawbacks that wipe them out faster.
For CTOs, CCM is a systems problem. Rules around eligibility, consent, concurrency, and supervision cannot live in training decks or tribal knowledge. They must be enforced through EHR logic, prompts, and locks that prevent errors before claims are generated.
The G0511 transition completed September 30, 2025. RHCs and FQHCs that prepared early are now realizing the upside of individual CPT billing. Clinics still defaulting to G0511 – or assuming the deadline was extended – should treat fixing the billing workflow as the highest-priority operational task this quarter.
At scale, the organizations that win are those that stop treating CCM as a billing workflow and start treating it as a data system. When care plans, time logs, and patient interactions are structured and interoperable, CCM becomes not just reimbursable but strategically valuable for quality reporting and value-based contracts.
Final insight: CCM codes are not billing artifacts. They are operational levers. When engineering, compliance, and finance align around them, CCM becomes a predictable engine for revenue stability, audit readiness, and value-based care performance.
Verified via primary CMS sources + industry confirmation 2026-05-02:
- CMS CY 2025 Medicare Physician Fee Schedule Final Rule (issued November 1, 2024) – established the original G0511 transition window January 1, 2025, through July 1, 2025. CMS fact sheet. Verified 2026-05-02.
- CMS Medicare Learning Network newsletter (June 5, 2025) – extended G0511 billing allowance through September 30, 2025. NARHC summary of regulatory wins. Verified 2026-05-02.
- Final sunset: September 30, 2025. As of October 1, 2025, RHCs and FQHCs must use individual CCM CPT codes (99490, 99439, 99487, 99489) – G0511 is no longer reimbursable.
No. Non-complex CCM (99490/99439) and complex CCM (99487/99489) cannot be billed for the same patient in the same calendar month. Practices must choose the code family that best reflects the patient’s acuity, documented medical decision-making, and total time. Billing both will trigger denials and may expose the account to audit.
Yes, but only if the service periods do not overlap. TCM (99495 or 99496) covers the first 30 days following discharge. CCM time may only begin after day 30. If CCM minutes are logged during the TCM window, payers will deny the CCM claim. EHR data controls are the safest way to enforce this rule.
Only the physician or qualified health professional may count time toward 99491 and 99437. Clinical staff time cannot be included. Documentation must clearly reflect personal provider involvement and exclude staff activities. These codes are reimbursed at higher rates and are reviewed more closely.
No. G0506 is optional. It may be billed when the practitioner personally performs extensive care planning during the initiating visit. CCM services can still begin without G0506, provided eligibility, consent, and a care plan are properly documented.
Rural Health Clinics and Federally Qualified Health Centers may continue using G0511 through September 30, 2026. After that date, they must transition to individual CCM CPT codes such as 99490, 99439, 99487, and 99489. Organizations should update workflows and train coding teams ahead of the deadline to avoid revenue disruption.
Yes, but with limits. CCM may be billed with either RPM or RTM, not both at the same time. If both monitoring programs are active concurrently, CCM claims are at risk for denial. System-level checks are recommended.
The most frequent audit gaps include missing patient consent, incomplete care plans in certified EHRs, weak documentation of moderate or high medical decision-making for complex CCM, and unclear separation between staff time and physician time. Addressing these gaps proactively reduces the risk of recoupment.


